

Article
Related Links
Michael Dienst,*† MD, Patrick E. Greis,‡ MD, Benjamin J. Ellis,§ Kent N. Bachus,ll PhD, and Robert T. Burks,‡ MD
From the †Department of Orthopaedic Surgery, University Hospital, Homburg/Saar, Germany, ‡Department of Orthopaedic Surgery, University Hospital, Salt Lake City, Utah, §Scientific Computing and Imaging Institute, Musculoskeletal Research Laboratories, University of Utah, Salt Lake City, Utah, and llOrthopaedic Research Laboratory, University of Utah, Salt Lake City, Utah
Background: A mismatch of the original lateral meniscus and a lateral meniscus allograft by inaccurate preoperative radiographic sizing can have significant consequences on ultimate function.
Hypothesis: The size of a lateral meniscal allograft affects the contact mechanics of the femoral condyle on the tibial plateau.
Study Design: Controlled laboratory study.
Methods: Four right and 2 left knees were tested as intact joints, after meniscectomy, and after replantation with the original menisci and 16 right or 9 left human, fresh-frozen lateral meniscal allografts, respectively. The allografts were allocated into 7 groups according to their outer and inner anteroposterior and mediolateral diameters. Biomechanical testing was performed as compressive loadings with constrained motions in extension and 30° of flexion. Measurements were done with Fuji pressuresensitive films for contact parameters of the direct femorotibial and meniscotibial contact.
Results: Oversized lateral meniscal allografts led to greater forces across the articular cartilage, whereas undersized allografts resulted in normal forces across the articular cartilage but greater forces across the meniscus. Two undersized transplants failed. Most of the contact parameters of allografts 10% smaller or larger than the original menisci were in the range of the intact knees. The knees after meniscectomy showed greater forces of the direct femorotibial contact areas than did the intact knees and the knees with the replanted original menisci. The contact mechanics of the knees with the replanted original menisci were close to normal.
Conclusion: The size of a lateral meniscal allograft has a significant effect on the contact mechanics of the tibial plateau.
Clinical Relevance: Preoperative radiographic sizing needs to be performed precisely to identify a suitable lateral meniscal allograft. A mismatch may be the reason for failure of the allograft or subsequent development of degenerative changes. A mismatch on graft selection of less than 10% of the size of the original meniscus may be acceptable.
Keywords: knee; meniscal allograft; transplantation; meniscal sizing
Various factors affecting the results of meniscal allograft transplantation have been reported. It has been shown that the midterm and long-term results are significantly affected by the initial condition of the articular cartilage and ligamentous stability.21 Cadaveric studies have demonstrated that the surgical technique influences the biomechanical situation. Anatomical and secure fixation of both the anterior and posterior horn of the allograft is necessary to restore contact mechanics close to normal.1,3,14 Biomechanics are also influenced by the transplant material itself. Neither a lyophilized nor a deep-frozen meniscus reaches the tensile strength of normal meniscal tissue; however, the deep-frozen meniscus has higher strength than does the lyophilized transplant.11
Accurate sizing and positioning of a meniscal allograft have been reported as other important factors for a successful outcome of meniscal transplantation.4,5 However, reliability of preoperative radiographs or MRI for sizing of the meniscal allograft is variable.14,15,19 Using even less stringent criteria for accuracy, radiography or MRI was 79% or 83% reliable, respectively.19 Sekaran et al18 have shown that placement of the posterior horn tunnel in a nonanatomical location caused a significant alteration of the contact pressure distribution of the knee. Thus, better understanding of the tolerance for meniscus size and positioning mismatch is necessary.
Multiple surgical techniques have been used for medial and lateral meniscal transplantation. For lateral meniscal allograft transplantation, many surgeons use a lateral meniscal allograft with a single bone bridge attached to both the anterior and posterior horns.22 Fixation is done via a trough or a keyhole created in the lateral tibial plateau using transosseous suture fixation or press-fit fixation, respectively. A unique feature of this technique may be the fixed size of the allograft. In contrast to a single bone plug or suture-only fixation into separate bone tunnels, the allograft size cannot be adjusted by pulling the horns of the allograft into the tunnels. Thus, accurate preoperative sizing of the lateral meniscal transplant appears crucial to achieve a transplant of equal size to the original lateral meniscus (OM). A mismatch of the allograft and OM size may be the reason for early failure of transplantation, such as a rupture of the allograft, or the cause of progressive deterioration of the joint. Most authors report more than half of their transplant failures within the first 4 years after transplantation.12,16,2
It is unknown whether the size of the meniscal allograft affects the contact variables of the tibial plateau. The objective of this study was to determine whether the contact variables with a lateral meniscal transplant of a size similar to the OM were different from those with transplants of smaller or larger menisci.
MATERIALS AND METHODS
Cadaveric Knees and Meniscal Allografts
Thirteen human, fresh-frozen cadaveric knees were used for testing in this study. Anteroposterior and lateral radiographs were obtained of each knee for assessment of signs of osteoarthritis. After the specimens were thawed overnight at room temperature, arthroscopy of the cadaveric knees was performed for identification of meniscal tears and cartilage degeneration. Five knee joints had to be excluded from the study because of meniscal tears of the medial or lateral meniscu
s or radiographic or arthroscopic signs of osteoarthritis (cartilage degeneration worse than IIA13). Two knee joints had to be excluded during testing because of a fracture of the femoral metaphysis and a progressive insufficiency of the ACL. Six cadaveric knees (4 right and 2 left) from 5 women and 1 man (mean age, 66 years; range, 49-79 years) were included in this study.
Sixteen right and 9 left human, fresh-frozen lateral meniscal allografts were obtained from a tissue bank (Cryolife Inc, Marietta, Ga). Age and gender of the transplants were not known. Macroscopic inspection and palpation of the transplants showed intact menisci without any signs of degenerative changes, and each was still attached to a complete lateral tibial plateau.
Preparation of the Cadaveric Knees and Meniscal Allografts
Each knee was prepared by transecting the femur and the tibia about 25 cm from the joint line. Both the femur and the tibia were potted in hollow, cylindrical tubes with low melt. The lateral compartment was accessed via a lateral parapatellar arthrotomy. The subsequent lateral femoral condyle osteotomy was planned as a vertical cut starting directly lateral to the femoral origin of the ACL aiming to the lateral transition of the femoral diaphysis and metaphysis.10 Two 8-mm tunnels were drilled perpendicular to the planned osteotomy plane. The tunnels were filled with polymethyl methacrylate (PMMA), which was threaded for introduction of 6-mm threaded rods. The threaded tunnels of the condyle fragment were overdrilled to 7 mm for compression of the condyle during relocation (Figure 1). The defect of the saw blade was compensated for with a Teflon film.

Figure 1. Relocated osteotomy of the lateral femoral condyle. The defect of the saw blade is compensated for with a Teflon film.
For orientation of the pressure-sensitive film for later analysis of the films, 2 bone tunnels were drilled from the tibial metaphysis to the posterolateral and anteromedial lateral tibial plateau. Two guide wires were introduced and advanced underneath the surface of the articular cartilage.
After the intact knee was tested, the OM was removed. For later anteroposterior and mediolateral orientation of the lateral meniscus allograft, the tip of the lateral eminence was marked. The lateral condyle was dissembled and the meniscocapsular junction dissected. Using small osteotomes, we removed the meniscus, with both horns adherent to a small bone bridge. Exactly half of the tibial eminence was removed with the bone bridge, so that the lateral half with the mark was left attached to the lateral tibial plateau. The tibial defect was further depressed and filled with PMMA. A plastic block of a size slightly bigger than the bony meniscal bridge was used to mold a box into the cement (Figure 2). The block was flush with the lateral half of the tibial eminence to avoid fixation of the transplant in a nonanatomical medial position. During the molding process, the anteroposterior position of the lateral eminence was marked on the plastic block. At the same anteroposterior position, a thread was cut into the bottom of the box for a 4.5-mm cortical screw (Figure 2).
. A thread was cut into the bottom of the box for screw fixation of the bone block (arrow).")
Figure 2. Cement box preparation for implantation of the original lateral meniscus and lateral meniscal transplants. The lateral rim of the box was bounded by the tip of the lateral tibial eminence (black mark). A thread was cut into the bottom of the box for screw fixation of the bone block (arrow).
The explanted OM and the allografts were dissected from soft tissues and measured (Figure 3). In comparison to the size of the OM, the allografts were separated into groups according to their size either by the mean of anteroposterior and mediolateral outer diameter or by the mean of the anteroposterior and mediolateral inner diameter. In comparison to the OM, the menisci of group “XXS” and “XXL” were at least 17.5% smaller or bigger, respectively. The menisci of groups “XS” and “XL” were between 10.5% and 17.5% smaller or bigger, respectively, and the menisci of groups “S” and “L” were between 3.5% and 10.5% smaller or bigger than the OM, respectively. The menisci of group “0” were in the range of ±3.5% of the size of the OM.

Figure 3. Measurement of the original lateral menisci and lateral meniscal transplants. OD, outer diameter; ID, inner diameter; ml, mediolateral; ap, anteroposterior.
The bone bridges of the OM and allografts were trimmed back to fit into a negative of the plastic block identical to the box in the tibial plateau. Laterally, the bone bridge of the allografts was trimmed back to the tip of the lateral eminence. Proper mediolateral and anteroposterior alignment in the box was achieved by contact of the tip of the cut-in-half tibial eminence and the mark on the negative. Thus, for larger allografts, the horn locations moved farther apart, and for smaller allografts, the horn locations moved closer together. The menisci were then potted into the negative with PMMA and removed. A 4.5 drill bit was used to drill a hole into the center of the meniscal bone block/cement block at the position of the lateral tibial eminence. Reimplantation was done by compression screw fixation of the meniscal block into the box of the tibial plateau (Figure 4). The outer edge of the menisci was sutured to the capsule using single, vertical loop stitches of a 2-0 Ethibond braided suture (Ethicon Inc, Johnson & Johnson, Somerville, NJ) spaced 10 mm apart. The osteotomy was reassembled.

Figure 4. Fixation of the meniscal transplant in the cement box with a compression screw. Proper anteroposterior and mediolateral orientation was achieved by contact of the tip of the lateral tibial eminence (black mark).
Testing
Biomechanical testing was performed with a universal testing machine (858 Bionix Test System, MTS Systems Corp, Eden Prairie, Minn). The femoral cylinder of each knee joint was mounted into custom fixtures that allowed the knee to be fixed at 0° and 30° of flexion. Rotation was fixed with the patella facing parallel to the transepicondylar line. Depth of the cylinder was set so that the distance to the upper center of rotation was the same as the distance to the distal center of rotation measured from the joint line of the knee. The tibial fixation rig allowed flexion, rotation, and varus-valgus angulation.
Each knee joint was tested with the joint intact (INT), with the replanted OM, after meniscectomy (NM), and with each of the right or left meniscal allografts. Each knee was removed from the testing machine only between conditions INT and OM. For testing of the OM and the allografts, the knee was kept in the machine; the
OM and allografts were removed and replanted after dissembling and reassembling of the osteotomy only. Each condition was tested in full extension and 30° of flexion only (Figure 5). Analysis of the literature revealed that the contact parameters show no significant differences between 15° and 60° of flexion.1-3,10,14,18
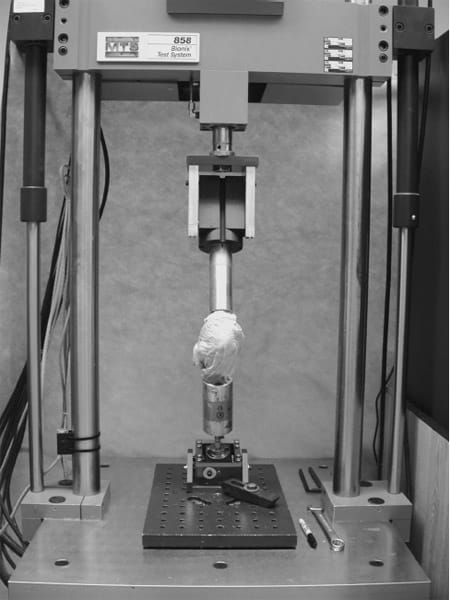
Figure 5. Knee specimen mounted into the testing machine (30° of flexion).
Preconditioning was performed by 3 loadings of the specimen with the testing protocol. For the first 2 preconditioning cycles, rotation and varus-valgus angulation of the tibial rig were unlocked. At the last preconditioning cycle, both directions were locked during the maximum load of 1000 N. Contact area and pressure were measured using a 2-layered, pressure-sensitive film (Super-Low Range Fujifilm Prescale Indicating Film, SPI, East Hanover, NJ).9 Custom-sized, 0.25-mm-thick polyethylene film packets were prepared from a template of the lateral tibial plateau. A braided suture was incorporated to the medial margin of the film packet for introduction of the films via a small perforation of the posterior capsule. Under slight distraction of the knees, the film packets were pulled under the menisci before the anterior horn sutures were closed. Loading of the knee joints was increased over a linear ramp to 1000 N for 17 seconds, held over a plateau for 5 seconds, and released.1,2 At the plateau phase, the two 1.5-mm pins were shortly advanced to stain the pressuresensitive film for later orientation. Each compressive loading was performed 5 times. Two films with higher noise or scratches were excluded; thus, 3 films for each condition and position were used for further evaluation.
Data Analysis
A calibration curve for the film was generated.1,9 The dyereceiving layers of the knee-exposed film packets were scanned simultaneously with a high-resolution scanner. A digital picture of the tibial articular surface of each knee joint was taken. For the following graphical preparation and analysis, Adobe Photoshop software (Adobe Systems Inc, San Jose, Calif) was used. The digital pictures of the tibial surfaces were rotated until the line connecting the posterior edges of the medial and lateral articular surfaces was oriented horizontally. After thresholding of the scans, the single scans of the film packets were copied in the pictures of the tibial surfaces, sized, and oriented using the holes of the 2 small 1.5-mm wires of the tibial surface and the corresponding dots on the pressure-sensitive films (Figure 6). Each scan was placed on a new layer, superimposing the image of the plateau.

Figure 6. Graphical superimposing of the film scans on a digital picture of the tibial plateau using the marker tunnels of the plateau and corresponding dots on the films.
From each layer, the same rectangular area was copied into a new file. The upper limit of that area was defined by the horizontal, posterior articular line (x-axis, y = 0); the lateral limit was defined by the lateral margin of the articular surface (y-axis, x = 0). Thus, an identical coordination system was defined for each film. The limits of the cartilage of the lateral tibial plateaus were marked and transferred to each file of the single scans. The following parameters were graphically marked with a graphic table board: the direct contact area between the articular cartilage surfaces of the lateral femoral condyle and the lateral tibial plateau (AFC), the mean pressure of the direct contact area (PFC), the peak pressure of an area of 0.3 cm2 (PFC0.3cm2), the peak pressure of an area of 0.1 cm2 (PFC0.1cm2), the mean pressure of the area of the articular surface of the lateral tibial plateau minus AFC (PMen), and the x and y locations of the maximum pressure (Figure 7).
; PMEN, mean meniscotibial pressure.")
Figure 7. Measurement parameters on the pressure-sensitive films. AFC, femorotibial contact area; PFC, mean femorotibial contact pressure; PFC0.3cm2 and PFC0.1cm², peak pressures of the femorotibial contact; x and y, location of the maximum pressure (arrows); PMEN, mean meniscotibial pressure.
Descriptive statistical analysis was performed using box diagrams for illustration of the differences between the groups INT, OM, and NM and the groups of different allograft sizes. For statistical analysis of differences between the groups, a t test for unpaired samples was used (significant at P <.05). Linear regression analysis (Pearson) was performed for evaluation of a linear dependency of the size of the meniscal transplant and the contact parameters (significant at P <.05).
RESULTS
Comparison Between INT, OM, and NM
Nondestructive results
In extension and at 30° of flexion, the mean pressure PFC and the peak pressures PFC0.3cm2 and PFC0.1cm2 for the knees NM were greater than for the INT and the knees with the replanted OM (Figures 8-11). These differences were significant in extension and bigger for the peak pressures. For both extension and flexion, there were only slightly higher pressures for PFC, PFC0.3cm2, and PFC0.1cm2 in OM than in INT without a significant difference. The pressure PMen was significantly smaller in NM and OM knees than in INT knees.
For both extension and flexion, the contact area AFC for the INT was smaller than for the knees with the replanted OM, and AFC for the knees with the replanted OM was smaller than for the knees NM (Figures 12 and 13). These differences were not significant. After meniscectomy, the center of the contact area was shifted laterally 1.1 mm and 1.9 mm in extension and flexion, respectively, and shifted anteriorly 0.9 mm in extension and posteriorly 4 mm in flexion. These shifts were not significant.
Comparison Between the Different Allograft Sizes
A significant increase of PFC, PFC0.3cm2, and PFC0.1cm2 was seen with increasing size of the allografts in extension (Figures 8 and 10). On the other hand, PMen significantly decreased. PFC, PFC0.3cm², and PFC0.1cm² in allografts of the group “XXL” were significantly higher than in INT. On the other side, PMen was significantly smaller in allografts of the group “XXL” than in INT. Some of the measured pressures for the allografts of sizes smaller than “S” were significantly smaller for PFC, PFC0.3cm², and PFC0.1cm² and bigger for PMen than in the knee NM. Most of the measured pressures of the groups “S,
” “0,” and “L” were in the range of the INT knees and knees after replantation of the OM. In flexion, the differences were less significant (Figures 9 and 11). The tendency was similar to the results at extension; a significant difference in comparison to the INT knees was found for PMen in “XXL” only.
, knees with the replanted original meniscus (OM), and knee after meniscectomy (NM) and for the different allograft groups after allocation from the mean of their outer diameters in extension. *pNM < .05. +pINT < .05. xpINT < .05. Linear regression analysis: pFFK = .032. pFFK0.3cm² = .022. pFFK0.1cm² = .033. pFMen = .003. See text for complete description of abbreviations.")
Figure 8. Contact pressures for the intact knees (INT), knees with the replanted original meniscus (OM), and knee after meniscectomy (NM) and for the different allograft groups after allocation from the mean of their outer diameters in extension. *pNM < .05. +pINT < .05. xpINT < .05. Linear regression analysis: pFFK = .032. pFFK0.3cm² = .022. pFFK0.1cm² = .033. pFMen = .003. See text for complete description of abbreviations.
, knees with the replanted original meniscus (OM), and knee after meniscectomy (NM) and for the different allograft groups after allocation from the mean of their outer diameters in flexion. +pINT < .05. See text for complete description of abbreviations.")
Figure 9. Contact pressures for the intact knees (INT), knees with the replanted original meniscus (OM), and knee after meniscectomy (NM) and for the different allograft groups after allocation from the mean of their outer diameters in flexion. +pINT < .05. See text for complete description of abbreviations.
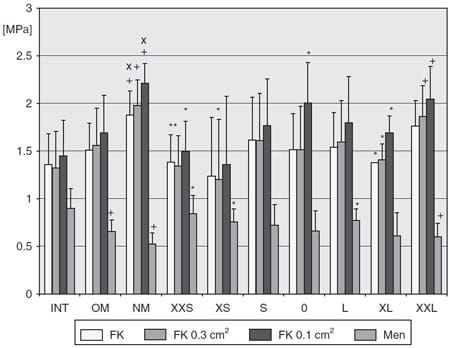
Figure 10. Contact pressures for the intact knees (INT), knees with the replanted original meniscus (OM), and knee after meniscectomy (NM) and for the different allograft groups after allocation from the mean of their inner diameters in extension. *pNM < .05. +pINT < .05. xpINT < .05. Linear regression analysis: pFFK0.3cm² = .044; pFFK0.1cm² = .033; pFMen = .039. See text for complete description of abbreviations.
, knees with the replanted original meniscus (OM), and knee after meniscectomy (NM) and for the different allograft groups after allocation from the mean of their inner diameters in flexion. *pNM < .05. +pINT < .05. xpINT < .05. See text for complete description of abbreviations.")
Figure 11. Contact pressures for the intact knees (INT), knees with the replanted original meniscus (OM), and knee after meniscectomy (NM) and for the different allograft groups after allocation from the mean of their inner diameters in flexion. *pNM < .05. +pINT < .05. xpINT < .05. See text for complete description of abbreviations.
For both extension and flexion, the contact area AFC increased with larger sizes of the allografts (Figures 12 and 13). Linear regression analysis revealed a significant increase for outer diameter in flexion and for inner diameter in extension. In extension and flexion, the center of the contact area was shifted laterally with increasing sizes of the allografts. There was a significant linear correlation in flexion.
, knees with the replanted original meniscus (OM), and knee after meniscectomy (NM) and for the different allograft groups after allocation from the mean of their outer diameters. *pNM < .05. Linear regression analysis: pFlexion = .008.")
Figure 12. Contact areas AFC in flexion and extension for the intact knees (INT), knees with the replanted original meniscus (OM), and knee after meniscectomy (NM) and for the different allograft groups after allocation from the mean of their outer diameters. *pNM < .05. Linear regression analysis: pFlexion = .008.
, knees with the replanted original meniscus (OM), and knee after meniscectomy (NM) and the different allograft groups after allocation from the mean of their inner diameters. Linear regression analysis: pExtension = .045.")
Figure 13. Contact areas AFC in flexion and extension for the intact knees (INT), knees with the replanted original meniscus (OM), and knee after meniscectomy (NM) and the different allograft groups after allocation from the mean of their inner diameters. Linear regression analysis: pExtension = .045.
During testing, 2 lateral meniscal allografts in the group “XXS” failed. One rupture occurred during flexion at the posterior horn, and the other allograft failed at the anterior horn during extension.
DISCUSSION
Interpretation of Results
The purpose of this study was to determine whether the contact variables with the lateral meniscal allografts of different sizes were different from the contact variables with the lateral meniscal autograft or lateral meniscal allografts of similar sizes to the OM. The key findings were that (1) the replanted autografts did restore the contact mechanics only close to normal, (2) there was a significant correlation between the size of the allograft and the contact mechanics of the tibial plateau, (3) allografts sized 17.5% bigger than the OM showed significantly higher contact pressures than did the OM, and (4) allografts sized 10.5% smaller than the OM showed increased forces in the meniscus and thus may be predisposed to early failure.
Analysis of the contact mechanics showed only a slightly nonsignificant increase of the direct femorotibial contact pressures of the knees with the autografts (OM) compared with the INT. The differences were more obvious in extension. Here, the mean contact pressure (PFC) increased by a mean of 0.15 MPa. The knees with the replanted autografts showed significantly smaller or a trend for smaller contact pressures than did the knees NM in extension and flexion, respectively. These findings are similar to the results of other studies. Chen et al3 showed that both autografts with a bony bridge and autografts with both horns secured gave similar results to those for the INT. Alhalki et al1 found that the contact pressures of autografts replanted with bone plug fixation were close to normal; however, the peak pressure was significantly higher than in the intact knees. These findings were also more prominent in extension.
The results from this study showed that the direct contact area between the cartilage of the lateral femoral condyle and the lateral tibi
al plateau (AFC) was not significantly different for the INT, the knees with the replanted autografts, and the knees NM for both extension and flexion. There was even a trend for larger contact areas for the replanted OM and the knees NM. This is in contrast to other studies. Chen et al3 and Alhalki et al1 found a significant decrease of the contact area of up to 50% for the knees NM compared with the INT knees. This must be related to a different area selection. In the present study, only the direct contact area between the cartilage of the femoral condyle and the tibial plateau was traced. The less intense and irregular staining of the contact between the meniscus and the tibial plateau was not included. Thus, if the meniscus were removed or an oversized allograft were used, the contact area should be bigger. This was the case in the present study: the contact areas increased with the size of the meniscal allografts.
The film analysis in the present study included a new parameter (PMen): the area of the tibial plateau minus the direct femorotibial cartilage contact area. The mean pressure of this area was defined as the simplified pressure transmitted via the meniscal tissue. The film analysis revealed a significant pressure reduction for the knees with the replanted autografts and the knees NM for both extension and flexion. This was consistent with the results for the meniscal allografts. There was a significant negative correlation of the pressure transmitted via the meniscal tissue and the size of the meniscal allograft for both extension and flexion. Thus, the bigger the allograft, the less the load transmission via the meniscal tissue. Conversely, the load transmission via the meniscal tissue increased with smaller size of the meniscal transplants.
Thus, even reimplantation of the OM does not fully restore the normal function of the meniscus. This is probably related to dissection of ligaments at the horn insertion site, of ligaments between the menisci (Lig intermeniscale), and of other ligaments such as the ligaments of Humphrey and Wrisberg, which are not restored during transplantation.17 Biomechanical studies have shown that a compressive force applied to the knee joint generates radially directed forces that, because of the bone attachment at both horns, produce hoop stresses in the meniscus. 3,7 Thus, a secure horn fixation is most important to withstand these hoop stresses.1,3,14 It may be speculative, but the 2 failures of this study with ruptures at the horn sites of very small allografts likely indicate that smaller allografts are at risk for rupture. The hoop stresses in small allografts are likely too high, leading to either rupture of the meniscal horn tissue or failure of the horn fixation. This may be a cause for early failures of meniscal transplantation in vivo.
Analysis of the pressure of the direct cartilage contact between the femoral condyle and the tibial plateau of the meniscal allografts revealed a significant correlation between the size of the allograft and the mean and peak pressures for extension and flexion, respectively. In extension, the contact pressures were significantly higher for the allografts of much bigger sizes than the autografts. The contact pressures of allografts 10.5% or more smaller than the autografts were similar to those of the intact knees. The contact pressures of allograft with sizes of a mean of 7% to –7% were similar to those of the autograft. Thus, with respect to the direct femorotibial cartilage contact areas, smaller allografts would restore the contact pressure closer to normal. However, as indicated in the previous paragraphs, a possible higher risk for failure of the meniscus transplant has to be taken into consideration if smaller allografts are used.
The center of the contact area was shifted laterally with increasing size of the allograft. This was significant only in flexion. Sekaran et al18 found a significant posterior shift of the center of the contact area with both a medial and posterior nonanatomical position of the posterior horn tunnel in medial meniscal transplantation. A transverse shift was not observed. It has to be considered that only autografts were tested in that study and that the experiments were done with medial menisci. Thus, the anterior horn position and size of the menisci were not altered. Moreover, the posterior horn of the medial meniscus has been highlighted as an important restraint to anterior displacement of the tibia, especially in anterior cruciate deficiency.8 In the present study, the menisci were positioned in the anatomical anteroposterior position; thus, a significant anterior or posterior shift in a stable joint would have been unlikely. Moreover, the lateral meniscus is not as important an anteroposterior stabilizer as is the medial meniscus. 8 However, our observation of a significant lateral shift in the knees NM and with increasing allograft size in flexion only may indicate a role of the lateral meniscus as a mediolateral stabilizer when the collateral ligaments and the articular capsule are not tight.
Methodological Issues
The distribution of allografts into different groups by their anteroposterior and mediolateral dimensions was based on studies on the accuracy of preoperative sizing. Shaffer et al19 showed that the mean difference between radiographic measurements and actual meniscus dimensions was 2.35 mm. Magnetic resonance imaging measurements were only slightly more accurate with a mean difference of 2.25 mm. Considering an anteroposterior length and mediolateral width of the lateral meniscus with a mean of 36.6 ± 6.1 mm and 26.8 ± 2.96 mm, respectively,19 the error of preoperative radiographic sizing would be between 6.4% and 8.8%. These values were confirmed by Pollard et al,15 who determined an error of preoperative radiographic sizing of the lateral meniscus of 7.4%. Thus, only 70% to 80% of the menisci sent from the tissue bank would be in a size range of ±10% of the OM. However, similar to the definition of Shaffer et al,19 the measurements of an “ideal” graft should fall within ±1 mm of the actual anatomical dimensions. Thus, for the present study, an “ideally sized” allograft (group 0) was defined with a size within ±3.5% (ca ±1 mm) of the size of the OM. Smaller and bigger allografts were distributed into the groups “L”/”S” (mean size difference, 7%), “XS”/”XL” (mean size difference, 14%), and “XXS”/”XXL” (mean size difference, 21%). Thus, if preoperative sizing was done accurately, allografts of the size groups S, 0, and L would be those to be sent by the tissue bank.
Access to the lateral compartment was achieved via osteotomy of the lateral femoral condyle. The same technique was used by other authors for osteotomy of the medial femoral condyle.2,10,18,19 Martens et al10 showed that osteotomy of the medial femoral condyle does not significantly change the pressure and contact area compared with those of the intact knee. In vivo, fixation of the bone block is usually done by transosseous sutures or press-fit fixation. With respect to the information of Alhalki et al1 of plug failures due to osteoporotic bone, the bone block between both meniscal horns was trimmed back to a small rim and potted into PMMA. To avoid loosening of the bone block in the tibial plateau, the box in the plateau was reinforced with PMMA. The compressive screw fixation allowed a stable fixation and fast change between the allografts. Moreover, the screw was always placed directly medial to the la
teral tibial eminence in the center of the PMMA-reinforced bone block. Thus, an accurate anteroposterior and mediolateral position of the allograft was secured. Sekaran et al18 showed that a nonanatomical placement of the posterior horn of a medial meniscal autograft adversely affects the pressure distribution on the tibial plateau.
A possible weakness of the present study may be that our model accounted for compressive load only. In contrast to the group of Hull and Howell,1,2,18 who used a 6 degrees of freedom load application system, motion was constrained during compression. However, unconstrained rotation and varus-valgus angulation were permitted during preconditioning and finally locked during the last maximum compressive load. Thus, smearing of the stain on the pressure-sensitive films was avoided, but shear and rotational forces were not accounted for. Similar models were used by other authors.3,14 Loading was limited to extension and 30° of flexion only. Analysis of the literature revealed that the contact parameters show no significant differences between 15° and 60° of flexion.1-3,10,14,18 With respect to complications at 60° of flexion during pilot studies, such as a progressive insufficiency of the ACL and a fracture of the femoral metaphysis, flexion was limited to 30°. It remains unclear how closely both single compressive load models and multiple degree of freedom load models replicate true in vivo properties and loading conditions.
The selection of a compressive load was based on other studies and the authors’ own experience during pilot studies. Ideally, the applied compressive load should have been about 1500 N (2 times body weight) to approximate the load across the knee during walking.6 However, Alhalki et al1 reported a failure of their bone plugs from the elderly, osteoporotic specimen at loads above 1000 N.We observed a fracture of the femoral metaphysis and avulsion of the ACL from the tibia during maximum compressive load. Thus, we used the same protocol as that of Alhalki et al.1,2 The compressive load was incrementally increased over 17 seconds until 1000 N was reached, held for 5 seconds, and released.
CONCLUSION
The results indicate that menisci of a size of ±10% of the OM restore the contact mechanics close to normal. From the data of our study, we suggest surgeons should select lateral meniscus transplants that are slightly larger rather than too small. Even if the contact mechanics of smaller allografts were closer to those of the intact knees than were allografts sized similar or larger than the OM, it appears likely that the use of smaller allografts predisposes to early failure of the operation. The observation of higher load transmission via the meniscal tissue in smaller allografts than in the replanted autografts and failure of 2 small allografts during testing leads to the suspicion that the hoop stresses may be too high and lead to rupture of the horn sites of the allografts.
To our knowledge, clinical investigations have not yet proven that meniscal transplantation can prevent further deterioration of the knee. The results of the present study indicate that the size of the allograft is another parameter that should be considered if the results of meniscal transplantation are analyzed.
ACKNOWLEDGMENT
The authors thank Todd Grunander, MD, and Daniel Ryssman,MD, for their help during the experiments of this study.
REFERENCES
- Alhalki MM, Howell SM, Hull ML. How three methods for fixing a medial meniscal autograft affect tibial contact mechanics. Am J Sports Med. 1999;27:320-328.
- Alhalki MM, Hull ML, Howell SM. Contact mechanics of the medial tibial plateau after implantation of a medial meniscal allograft: a human cadaveric study. Am J Sports Med. 2000;28:370-376.
- Chen MI, Branch TP, Hutton WC. Is it important to secure the horns during lateral meniscal transplantation? A cadaveric study. Arthroscopy. 1996;12:174-181.
- Garrett JC, Steensen RN. Meniscal transplantation in the human knee: a preliminary report. Arthroscopy. 1991;7:57-62.
- Johnson DL, Swenson TM, Livesay GA, Aizawa H, Fu FH, Harner CD. Insertion-site anatomy of the human menisci: gross, arthroscopic, and topographical anatomy as a basis for meniscal transplantation. Arthroscopy. 1995;11:386-394.
- Komistek RD, Stiehl JB, Dennis DA, Paxson RD, Soutas-Little RW. Mathematical model of the lower extremity joint reaction forces using Kane’s method of dynamics. J Biomech. 1998;31:185-189.
- Kummer B. Biomechanik des Meniskus. Orthopade. 1994;23:90-92.
- Levy IM, Torzilli PA, Warren RF. The effect of medial meniscectomy on anterior-posterior motion of the knee. J Bone Joint Surg Am. 1982;64: 883-888.
- Liggins AB, Finley JB. Recording contact areas and pressure in joint interfaces. In: Little EG, ed. Experimental Mechanics. Philadelphia, Pa: Elsevier; 1992:71-88.
- Martens TA, Hull ML, Howell SM. An in vitro osteotomy method to expose the medial compartment of the human knee. J Biomech Eng. 1997;119:379-385.
- Milachowski KA, Kohn D, Wirth CJ. Transplantation allogener Menisken. Orthopade. 1994;23:160-163.
- Noyes FR, Barber-Westin SD, Rankin M. Meniscal transplantation in symptomatic patients less than fifty years old. J Bone Joint Surg Am. 2004;86:1392-1404.
- Noyes FR, Stabler CL. A system for grading articular cartilage lesions at arthroscopy. Am J Sports Med. 1989;17:505-513.
- Paletta GA, Manning T, Snell E, Parker R, Bergfeld J. The effect of allograft meniscal replacement on intraarticular contact area and pressures in the human knee: a biomechanical study. Am J Sports Med. 1997;25:692-698.
- Pollard ME, Kang Q, Berg EE. Radiographic sizing for meniscal transplantation. Arthroscopy. 1995;11:684-687.
- Rath E, Richmond JC, Yassir W, Albright JD, Gundogan F. Meniscal allograft transplantation: two- to eight-year results. Am J Sports Med. 2001;29:410-414.
- Rijk PC, de Rooy TPW, Coerkamp EG, Bernoski FP, van Noorden CJ. Radiographic evaluation of the knee joint after meniscal allograft transplantation: an experimental study in rabbits. Knee Surg Sports Traumatol Arthrosc. 2002;10:241-246.
- Sekaran SV, Hull ML, Howell SM. Nonanatomic location of the posterior horn of a medial meniscal autograft implanted in a cadaveric knee adversely affects the pressure distribution on the tibial plateau. Am J Sports Med. 2002;30:74-82.
- Shaffer B, Kennedy S, Klimkiewicz J, Yao L. Preoperative sizing of meniscus allografts in meniscus transplantation. Am J Sports Med. 2000;28:524-533.
- Van Arkel ERA, De Boer HH. Survival analysis of human meniscal transplantations. J Bone Joint Surg Br. 2002;84:227-231.
- Wirth CJ, Peters G, Milachowski KA, Weismeier KG, Kohn D. Longterm results of meniscal allograft transplantation. Am J Sports Med. 2002;30:174-181.
- Yoldas EA, Sekiya JK, Irrgang JJ, Fu FH, Harner CD. Arthroscopically assisted meniscal allograft transplantation with and without combined anterior cruciate ligament reconstruction. Knee Surg Sports Traumatol Arthrosc. 2003;11:173-182.
