Article
Related Links
Participants: U.S. ARMY COMMUNICATIONS – ELECTRONICS COMMAND NIGHT VISION ELECTRONIC SENSORS DIRECTORATE U.S. ARMY INSTITUTE OF SURGICAL RESEARCH EXTREME TRAUMA STUDY BRANCH U.S. ARMY ABERDEEN TEST U.S. ARMY SOLDIER SYSTEMS COMMAND
Abstract
Research conducted by Department of Defense laboratories and facilities, collaborating with leading academic institutions, has demonstrated that currently available landmine protective footwear does not prevent severe injury. This footwear potentially reduces injury severity against some antipersonnel mines. Volume 2 of the Lower Extremity Assessment Program (LEAP 99-2) discusses the change of injury pattern in a cadaver model wearing mine protective footwear during an antipersonnel blast mine detonation. Our analytical methodology developed to assess mine-protective footwear and injury severity associated with blast mines across the spectrum of threat is presented.
Executive Summary
Landmine proliferation represents an ever-expanding global problem. More international organizations are becoming involved in demining operations. These efforts coupled with an expanding mine threat create a high potential for deminer injury in numerous regions worldwide increasing the need for better deminer protective equipment. This study was designed to assess the effectiveness of protective footwear during direct contact antipersonnel blast mine detonation.
This volume describes the medical aspects of landmine injuries in detail as they relate to clinical presentation and treatment. The medical significance of amputation level to potential outcome is described as a function of patient rehabilitation and cost.
The sharing of knowledge between the participants, combined with experimental trials, has led to a better understanding of the medical aspects of landmine injury and the elements of protective boot design that are clinically significant.
Past research led to recognition of the following requisites:
- Development of a biofidelic model of the lower extremity.
- Development of antipersonnel landmine-testing methodology.
- Medical assessment of injury severity.
Current testing demonstrates:
- Commercially available mine protective footwear does not prevent severe injury following landmine detonation.
- No further testing is necessary for the Wellco® Blast Boot and BFR® boots alone.
- Cadaveric testing is the most biofidelic model to accurately define the level of potential protection of any footwear. This method gives a reproducible method for AP mine injury assessment and should be utilized in future protocols.
- Mine blast injuries to the lower extremities do not directly correlate with current injury predictive curves developed by the automotive industry for cadaver testing.
Areas that require further investigation include:
- The effects of secondary missiles from the boot materials (metal attenuators) need to be evaluated by further testing on whole cadavers.
- The Med-Eng® boot demonstrated potential improvement in protection against the larger mines, but more testing is warranted due to the limited number of samples.
- Several nations (UK, Canada, Russia) have developed mine protective footwear employing various types of materials, standoff distance, and actuation mechanisms for protection. Evaluation of this new footwear using the testing methodology developed in this study is recommended.
- This study evaluated the protective footwear only. Additional testing will need to be performed to determine if there is any benefit or detriment to the lower extremity with the use of the Body Armor Set, Individual Countermine (BASIC) suit.
- The BASIC suit requires further testing to evaluate its limitations in protecting the wearer against the full range of antipersonnel landmine types and injury patterns (head, upper extremity, torso, contralateral limb, etc.).
- Due to the variability in live mine detonation, a mine surrogate utilizing cast and pressed TNT (based on threat mine prevalence) may give the most reproducible blast profile.
Foreword
This volume documents the detailed medical report of the injury patterns of the lower extremities produced by the M-14, PMA-2, and PMN antipersonnel mines as they relate to various levels of footwear protection. This volume addresses the effectiveness of the footwear based on medical diagnoses and treatment plans, the mechanism of injury and injury patterns associated with the different landmines tested, and builds on the information contained in Volume1.
Introduction
The first recorded use of explosive landmines occurred during the American Civil War with the invention of triggering mechanisms for “land torpedoes” by Confederate General Gabriel Raines (Time-Life Books, 1998). The introduction of tanks during World War I led to renewed interest in antitank mine development and current antipersonnel landmine design and employment techniques (Croll, 1998). Further refinement of landmine technology occurred during the Second World War, the first conflict to see large-scale use of landmines. Antipersonnel landmines have played a significant role in every major conflict since. In the 1970s and 1980s, numerous low intensity conflicts fuelled by Cold War rivalries led to a proliferation of landmine use.
This proliferation has led to a worldwide landmine problem of epidemic proportions. It is estimated that landmines kill 800 people per month and injure an additional 1200, amounting to 24,000 new victims per year (Landmine Survivor’s Network report, 1998). It is widely accepted that these are conservative figures, which do not reflect the actual number of casualties. Many victims never reach the medical treatment facilities where these statistics are compiled (Gray, 1997).
The presence of landmines has been shown to impede the economic and social rehabilitation of countries recovering from conflict. The safe use of productive farmland and valuable water sources can be denied to residents. When faced with starvation, communities are forced to cultivate mined areas often leading to worker injury. In agrarian countries, handicapped landmine victims are often unable to support themselves, becoming an economic burden on their families and war-torn communities. The International Committee of the Red Cross (ICRC) estimates the cost of providing a 10-year-old child with a lifetime of basic prosthetic limbs to be $3125 (Garachon, 1993).
Antipersonnel landmines are categorized into five groups as described by Taylor (1999).
- Blast: These are the most prevalent type worldwide and are usually surface laid or buried to a depth of 10-40mm. They are pressure activated and normally triggered by stepping on the mine. Protection from this type of mine is the goal of curren
t anti-mine footwear design. An example of this type of mine is the Soviet PMN mine (Banks, 1997). - Fragmentation: These mines rely on the explosive distribution of fragments from the shattered mine casing to create injury (Taylor, 1999). They are typically mounted above ground and tripwire activated. An example of this type of mine is the Soviet POMZ mine.
- Bounding fragmentation: These mines are a variant of the fragmentation mine. When activated, a propellant charge is ignited in the base of the mine causing the body of the mine to rise to a height of approximately one meter. A second fuse detonates the main charge distributing the fragments in a wider radius (Taylor, 1999). An example of this type of mine is the Soviet OZM-3.
- Directional fragmentation: This is a variant in which, the shape of the explosive charge determines fragment direction. These mines are designed to direct their explosive charge; usually in a fan, in the general direction determined by the operator. The fragments are normally pre-formed objects, such as ball bearings, which are set in a resin matrix. An example of this type is the U.S. M18A1 “Claymore” antipersonnel mine.
- Shaped charge: This type of mine is a variation of the blast mine, also pressure activated, in which the explosive force is directed by the shape of the charge. Although very rare, this mine type is designed to overcome protective measures. The Canadian C3A2 “Elsie” is an example is the (Taylor 1999).
Typical blast mines can be roughly grouped into three categories based on explosive weight:
- Small: Explosive weight of 25 – 50 grams
- US M-14, 28 grams
- Chinese Type 72, 34 grams
- Yugoslav PMA-3, 35 grams
- Medium: Explosive weight of 50 – 150 grams
- Soviet PMN-2, 100 grams
- Yugoslav PMA-2, 100 grams
- Large: Explosive weight of over 200 grams
- Soviet PMN, 240 grams
- Yugoslav PMA-1A, 200 grams
Most AP blast mines are pressure-operated devices, utilizing a mechanical fuzing system that initiates the main charge. Some mine cases are plastic, others are cased in wood while metallic casings are less common. A majority of mines are cylindrical in shape with a pressure plate bearing on an internal fuse or spigot fuse protruding from a central well. Activating pressure can be as low as 2 kg. Most mines use TNT (explosive power 3019 KJ/cm3g-1 – Taylor, 1999) as the main charge but some of the smaller mines use more powerful explosives such as Tetryl (explosive power 3675KJ/cm3g-1 – Taylor, 1999). Explosive geometry and density also contribute to energy potential. The combination of these factors makes it impossible to determine the relative explosive power of mines by explosive weight alone.
A blast mine is usually initiated by pressure on a fuzing mechanism, which detonates a booster or the main charge. Upon detonation, a small volume of explosive is converted into a large volume of hot gas. There is a resulting rise in pressure along a shock front resulting in a propagating “blast wind”, which is the primary injury mechanism. Particulate matter from the footwear, mine casing and from the ground can cause secondary fragment injury (King, 1969). The amount of secondary fragmentation is determined by the mine’s casing material, depth of burial, and the medium in which it is buried. The type of soil the mine is buried in has important effects as well. Heavy, wet soils are relatively resistant to blast propagation, thus directing more of the blast energy upward into the initiating limb, while soft soils absorb energy (The Technical Cooperation Program, 1998).
The use of landmines has long been restricted under International Humanitarian Law (Geneva 1998). Recent efforts have sought to completely ban the use, stockpiling, production, and transfer of anti-personnel landmines. One hundred and fifty-three countries signed the Ottawa Treaty of 1997 and seventy-one have ratified it as of 31 March 1999 (International Humanitarian Law, 1998). Landmines continue to be used in contemporary conflicts despite international treaties banning their use.
In response to the global landmine epidemic, the United Nations and other non-governmental organizations (NGOs) have initiated demining programs. Although several techniques for clearing mined areas exist (vehicles, dogs, etc.), human deminers remain the most reliable and effective means. This method however, is quite dangerous and exposes the deminer to the risk of severe injury or death. In the aftermath of World War II, one deminer was killed or injured per 3279 mines cleared (Bowyer, 1996). For current humanitarian demining programs, preliminary data suggests that approximately 100 deminers are injured per year (Landmine casualty data report: Deminer injuries, 2000).
To better protect US soldiers operating in mined areas, the United States Army Infantry School developed a written requirement for footwear capable of defeating the M-14 antipersonnel landmine. The U.S. Army Test and Evaluation Command, U.S. Army Soldier Systems Command, and Aberdeen Test Center (ATC) were involved in the initial mechanical testing of the footwear produced for the Body Armor Set, Individual Countermine Pre-planned Product Improvement (BASIC P3I) (U.S. Army Yuma Proving Ground, 1999). ATC was tasked to quantify the relative effectiveness of the footwear and conducted testing utilizing a mechanical leg construct. In an attempt to correlate the footwear’s blast attenuation properties to resultant medical outcomes, the U.S. Army Institute of Surgical Research, Extremity Trauma Study Branch (USAISR-ETSB) was enlisted in 1998.
Elements of this Department of Defense (DOD) interagency working group, designed a scientific research protocol called Lower Extremity Assessment Program (LEAP). Funded by the U.S. Army Communications and Electronics Command, Night Vision Electronic Sensor Development (CECOM-NVESD) for the purpose of humanitarian deminer protection, the USAISR-ETSB was tasked to evaluate the mechanism of injury and determine current levels of protection provided by commercially produced anti-mine footwear through correlation with medical outcomes.
Landmine protective footwear is designed to protect the lower extremity from proximity and direct contact explosions. Our study was designed to biomechanically evaluate blast landmine injuries and to correlate the medical outcomes based on various levels of footwear protection. The objectives for this study were:
- Provide data for the initial assessment of the effectiveness of mine protective footwear.
- Acquire strain and axial force measurements on a cadaver lower limb during anti-personnel mine detonations.
- Document the blast event.
- Provide empirical data for development of injury criteria.
Methods and Materials
The USAISR’s Institute Review Board in accordance with all Federal, State, and Local regulations, approved the LEAP protocol after review. In addition, the Medical Research Material Command Human Subject Review Board reviewed the protocol considering all ethical issues.
Twenty fresh-frozen full body human cadavers were obtained from the Willed Body Program at Southwestern Medical Center in Dallas, Texas. All Federal, State, Local and Regulatory Commission rules were observed in the purchase, disclosure, transportation, and storage of the cadavers. Cadavers were maintained at -4 °C prior to testing and then thawed in a refrigeration unit maintained at 7.2 °C for five days. The pretest radiographs of the lower extremity from the pelvis to the foot were performed to identify any preexisting pathology. Transportation to the range was in a refrigerated truck, where final instrumentation and testing took place. Before the test, the subject was clothed in Battle Dress Uniform
(BDU) and outfitted with the selected protective footwear. Following testing, the instrumentation was removed and the cadaver was returned to the USAISR and placed in cold storage until post-test radiographs and clinical dissections were completed.
The protocol specifications called for males = 70 years of age. However, due to availability issues, the study’s upper limit was 96 years of age, and two females were accepted for testing.
The Willed Body Program in accordance with all Federal, State, and Local regulations cremated the cadaver remains.
Various types and combinations of commercially available standard footwear and landmine protective footwear were evaluated and are listed in Table 1. The main objective of the study was to evaluate the level of protection of the Wellco® boots (study) compared to the standard combat boot (control). A small number of mines were tested against the BFR boot, Med-Eng boot, and improvised footwear to ascertain the potential effectiveness of these protective measures. The detailed descriptions of this footwear can be found in Volume 1 of this report. Figure 1 shows a cutaway of the Wellco® anti-mine footwear sole’s construction showing the V-shaped blast attenuation plate and aluminum honeycomb. The pre- and post-blast weights of the boots as well as fragment weights were recorded. Photographs and descriptions of the footwear post-blast are contained in this volume in Appendix D, Detailed Footwear Damage Assessments. Two specimens were tested in a striding position against PMN mines wearing the BASIC P3I pants to ascertain their potential benefit in contralateral limb injury reduction.

Table 1: Boot Types

Figure 1: BB Cutaway
Three different mine types were utilized for testing: the PMN, 240 g TNT (large); PMA-2, 100 g TNT (medium); and the M-14, 28 g Tetryl (small). They were selected to represent a sampling across the spectrum of AP mine threat worldwide. The detailed descriptions of the tested mines are contained in Appendix A of Volume 1 of this report.
Testing was conducted at a USAISR-ETSB Field Test Site. All shots were performed in a blast/biohazard containment shelter manufactured at ATC. Figure 2 shows the blast shelter. Cadavers were suspended from the ceiling using a specially designed harness constructed at the USAISR-ETSB. The mines were detonated in an 18” x 24” x 24” deep steel box constructed in the floor of the shelter. The shelter was elevated ~34” above ground level. Data collection equipment was housed in a mobile army surgical suite (ISO Shelter) shown in Figure 3.

Figure 2: Exterior View of the blast Shelter.

Figure 3: Data Collection ISO shelters.
The initial PMN test was uninstrumented in order to evaluate the injury patterns, facilitate the placement, and access instrumentation survivability in subsequent PMN tests. Load cells were used to measure force. Utilizing previous models from automotive tests, a four-inch segment was removed from the proximal tibia using a surgical saw (Stryker, Santa Clara, CA). The load cell fixture was potted into place using polymethyl methacrylate (PMMA, Richards, Memphis, TN) and further secured by drilling transversely through the bone and using 2-mm diameter stainless steel wires at the proximal and distal ends of the load cell. A polyethylene spacer was used to maintain alignment and stability of the limb for transportation to the field test facility. Once on site, the spacer was replaced with the appropriate load cell. The strain gauge was placed on the distal medial aspect of the tibia and on the lateral surface of the calcaneus as shown in Figure 4. Several load cells were used during the course of the study. A uniaxial load cell was used in LEAP 99-1 to measure force, but it was determined that more axes were needed to properly understand the mechanism of injury and thus for LEAP 99-2 multi-axis load cells were used. All force and strain measurement equipment is fully described in Volume 1 of this report.
Fuji® Prescale Film: Pressure-sensitive film (Sensor Products, Inc., Forest Hills, NY) was used between the foot and the inner boot as well as between the inner and outer boots in an attempt to quantify force transmission properties of the footwear.

Figure 4: Instrumentation Placement
No scoring system has previously been described which addresses the severity of landmine injury in this context. A new scoring system, the Mine Trauma Score (MTS), was developed to compare the severity of mine events under different test conditions. The MTS does not rely on the use of any physiological parameters in order to be applicable to the cadaver test model. The vast majority of landmine injuries in the field will require either transtibial or transfemoral amputations (Coupland, 1991). However, the scope of the MTS includes values appropriate to lesser degrees of injury, which allows for the evaluation of any protective effect of the footwear.
The following terms are defined for use in the MTS:
- Closed injury: Injury of the lower extremity that does not violate (lacerate, tear) the skin. There may be underlying fractures that will compromise functional outcome but the potential infective sequelae of injury may be avoided.
- Open contained injury: Any lower extremity in which the skin is breached (lacerated, torn) but little evidence of contamination is present. An example would be a laceration to the skin of a foot contained within an intact boot. By avoiding, the gross contamination usually associated with mine injury it is hypothesized that this group would sustain fewer complications such as infection.
- Open contaminated injury: Any blast mine injury to the lower extremity in which the skin is not only violated but the exposed soft tissue is visibly contaminated. This contamination may be from the soil, footwear debris, or mine fragments.
- Salvageable limb: A lower extremity in which the severity of the injury does not render primary amputation inevitable.
- Transtibial/transfemoral amputation. In some blast mine detonations, the injury will be of a severity to make it difficult to determine the level of amputation required. This occurs when the area of injury extends into the proximal third of the tibia. Even when the extent of soft tissue damage does not extend above the knee, there may be insufficient tibial stump to fit a workable prosthesis or there may be so much skin and muscle loss as to anticipate difficulties in delayed primary closure. In this circumstance, every attempt is made to keep the
- level of amputation transtibial for functional reasons. Revision to transfemoral may be required at a later stage. An MTS value of 3 represents this category of uncertainty of the final level of amputation.

Table 2: Mine Trauma Score System
Thirty-one mines were tested against various combinations of footwear for LEAP 99-2; seven mines were tested in LEAP 99-1, “Pilot Study” (PS1
-PS7). The test matrix is listed in Table 2. Before the test, the feet of the subject were outfitted with the various protective measures listed in Table 2. The load cell spacers were removed and replaced with the selected load cell. To prevent damage during transportation, the apposite strain gauges were implanted last. The strain gauges were attached to the cortical surface of each bone with fibrin glue after removing all tissue with acetone.

Table 3: Test Matrix
The specimen was suspended upright in a specially designed harness incorporating a modified Thoracic Lumbosacral Orthosis (TLSO) brace that stabilized the hips. The knee was fitted with an immobilizer to maintain axial alignment and simulate muscle rigidity.
The mines were employed flush with the surface of the dry sand in a steel box; similar to actual deployment. The heel of the boot was positioned directly over the anti-personnel blast mine in line with the tibia, with sufficient body weight to activate the mine. Case studies show there is substantial risk of injury to the contralateral limb during a mine event like the PMN. To mitigate this risk and prevent additional damage to the previously tested limb, smaller mines were used against the primary limb and then that limb was amputated prior to testing a PMN against the opposite limb. When testing the smaller mines the contralateral limb was secured in a flexed position away from the detonation and protected with Kevlar® fabric.
Explosive Ordinance Disposal (EOD) personnel using RP-80 commercial blasting caps armed the mines. Personnel from ATC, under direct supervision of EOD personnel, performed the firing and timing of data collection. This procedure and associated equipment are fully described in Volume 1 of this report. For the purposes of this study it is assumed that there is little variation in explosive profile between mines of the same type.
All explosive material was transported, stored, employed, and disposed of by Fort Sam Houston Explosive Ordnance Disposal (EOD) personnel in accordance with all Federal and DOD regulations. All range operations were performed in compliance with all DOD and Department of the Army regulations.
All personnel involved in the handling and instrumentation of the cadaveric specimens were trained in and utilized universal precautions. All cadavers were tested for communicable diseases before delivery from the Willed Body program. Cadaver preparation and testing facilities were cleaned and maintained in accordance with Brooke Army Medical Center (BAMC) operating room standard operating procedures.
Radiographic/cineradiographic procedures were conducted under approved Federal and DOD regulations and all range personnel were trained in safety procedures.
Weather data was obtained from the local weather station for the testing period. The temperature, barometric pressure, and relative humidity were reported for each day in three-hour blocks. The individual tests have been correlated to the specific period and the weather data specific to that time recorded in the database.
Before testing the cadavers underwent complete lower extremity evaluation to identify any preexisting pathology, and after testing to assess blast effects. Pretest radiographic assessments can be found in Appendix B, Pretest X-rays. The BAMC radiology department performed the following studies:
The cadavers were evaluated using Anterior-Posterior (AP) views of the pelvis, and AP and Lateral views of the femur, knee, leg, ankle, and foot. Complete lower extremity examination in 5-mm slices was conducted using a CT (Picker PQ 5000). MRIs were performed on the LEAP 99-1 cadavers, but after review by Orthopaedic traumatologists and a Radiologist, MRIs were deemed to be of no value in this type of cadaver testing and were discontinued.
For each specimen anatomical dissections were performed by one of two board-certified Orthopaedic Traumatologists blinded to the specific footwear and mine threat.
Force and Strain Data Collection was performed by personnel from ATC. All data collection methods and equipment used are fully described in Volume 1 of this report.
Photographic Data Collection was performed by personnel from ATC. All data collection methods and equipment used are fully described in Volume 1 of this report.
Photographs were taken of the cadaver just before detonation and again immediately following mine detonation.
Photographic Data: Personnel from ATC took high-speed video of all tests and the equipment used is fully described in Volume 1 of this report.
Personnel from ATC obtained high-speed radiographic images of each blast event. Methods and materials used are fully described in Volume 1 of this report.
Results
Twenty cadavers were utilized for thirty-eight total shots (Seven shots were conducted during LEAP 99-1). Two cadavers were female and eighteen were male. (Two females and two males were utilized during LEAP 99-1). The mean age of cadavers was 77 years with a range from 37 years to 96 years of age. The mean cadaver weight was 159 pounds with a range from 97 pounds to 205 pounds.
The weather data is on file in the LEAP 99-2 database maintained by the USAISR-ETSB.
A series of still photographs were taken of each cadaver just before and immediately following detonation. High-speed video was captured for all the tests and eight individual x-rays of the initial blast wave were captured for every shot (Cineradiography). All photographic data (still and high-speed) as well as cineradiographic images are on file at ATC and will be further addressed in Volume 3 of this report. All audiovisual images are on file at both ATC and the USAISR-ETSB.
The MTS value was assigned to each test cadaver by one of two experienced board-certified military Orthopaedic Traumatologists, each of who has a domestic practice consisting entirely of orthopaedic trauma. One surgeon gained field experience during the armed conflicts in Somalia and Haiti, the other in Bosnia and in treating Gulf War casualties. For the purposes of MTS evaluation, the surgeon was blinded to both the nature of footwear and the mine type in each case. Determination of the MTS value was done predominantly by inspection and dissection of the tissues; similar to the way it would be performed at initial surgery in the field. Post-test radiographs and computerized axial tomographs (CT scans) were also available for review during this process. In each case, the dissection was videotaped. An UK-trained Orthopaedic Surgeon who independently assigned MTS values reviewed the videotaped dissections. This surgeon gained extensive experience while engaged in humanitarian surgical programs treating landmine injuries in Afghanistan, Cambodia, Angola, Rwanda, and Sri Lanka. Interobserver agreement with regard to the independently assigned MTS values was 100%. The MTS values are listed in Table 4.
Fractures occurring at the cemented interface between the load cell and tibia were regarded as artifacts (occurring due to the presence of a stress riser at this point) and not taken into account in the MTS scoring. Furthermore, when surgical closure failure at the instrumentation site occurred, it was not graded as an open injury unless wound propagation was noted.

Table 5: Range of Injury Severities

Figure 5: Injury Comparisons M-14

Figure 6: Injury Comparisons PMA-2

Figure 7: Injury Comparisons PMN

Figure 8: Injury Comparisons Combat Boot

Figure 9: Injury Comparisons CB/OB

Figure 10: Injury Comparisons BB/OB
Selected force data is listed in Appendix E (Force Data). The detailed force data can be found in Volume 1 of this report. The Fuji film was either contaminated by body fluids or destroyed beyond evaluation in all cases.
Clinical dissections (Appendix A, Detailed Medical Assessments) were conducted following posttest radiographic evaluation. The posttest radiographic data (Appendix C, Posttest X-rays) and gross clinical examinations were both utilized in assigning MTS values.
The pre- and post-blast weights of the boots and remaining fragments were recorded. Post-blast digital photographs and descriptions of the footwear are contained in Appendix D, Detailed Footwear Damage Assessments. These data are on file at the USAISR-ETSB.
Detailed medical evaluations can be found in Appendix A. Example pretest radiographs can be found in Appendix B. Post-test radiograph can be found in Appendix C. Detailed boot damage assessments can be found in Appendix D.
The correlation analysis revealed that the boot and mine type were significant factors as well as the time to peak force. It was found that a significant increase in protection (p = 0.007) is obtained by using the over boot with either the combat boot or blast boot. Further, it was found that no statistical improvement in medical outcome is obtained by using the blast boot instead of the combat boot with the over boot. Analyses of the protective measures showed that no boot was able to reduce MTS score below the 2A threshold for the PMA-2 and PMN mines. The over boot in combination with the blast boot or combat boot is able to do this for the M-14 mine only. ANOVA revealed that the over boot combination significantly reduced the time to peak force (p = 0.031).
Each bone will be considered independently then the collective results will be used to evaluate the MTS.
Figure 11 shows the average value of calcaneus fractures that occurred with MTS for all mines. It is interesting to observe that a fracturing of the calcaneus is characteristic of the mine injury.

Figure 11: Calcaneus fracture by MTS.
Figure 12 shows the probability of navicular fracture occurrence that compared to the MTS. Fractures of the navicular were not observed for MTS less than 2A, and that a fracture of the navicular is characteristic of MTS of 3 or greater.

Figure 12: Navicular fracture by MTS.
Figure 13 shows that a fracture of the cuboid is characteristic of the MTS of 2 or greater.

Figure 13: Cuboid fracture by MTS.
Figure 14 shows that fracture of the talus follows the same trend as the navicular, with a talar fracture not occurring with a MTS less than 2A.

Figure 14: Talus Fracture by MTS
Fracture of the pilon area with respect to the MTS is shown in figure 15. Significant pilon fractures occur with higher MTS.

Figure 15: Pilon fracture by MTS.
Figure 16 shows the number of fractures that generally are associated with a mine injury.

Figure 16: Number of fractures associated with MTS.
Discussion
The purposes of our study were: a) to evaluate the relative protection offered by various combat and protective footwear; b) to determine the in-situ forces and strains experienced by the lower extremity under antipersonnel landmine blast conditions; c) to document the blast event; and d) medically evaluate the mine injury to the lower extremity that results from activation of a blast anti-personnel mine. Regardless of the degree of protection offered by the boot, it must be comfortable and permit the user to perform his routine tasks. For the manual deminer this includes squatting, lying in the prone position, and walking on uneven ground. Ergonomic aspects have not been considered in the LEAP study.
In an effort to reduce the level of trauma to the lower extremity from anti-personnel mines, attempts have been made to design protective footwear. In the early 1950s, the U.S. Marine Corps developed a 6-inch sabot attachment for the combat boot, while the Army evaluated protective shanks in the 1960s. Work conducted in the 1990s has led to the development of new anti-mine footwear. Before our study, anti-mine footwear has never been evaluated to determine its protective capability from a medical perspective.
Landmine injuries have reached epidemic proportions in third-world nations, and affect both combatants and civilians. From 1980 to 1993, the incidence of landmine-related injuries doubled, resulting in an estimated 2000 deaths or injuries per month (Landmine survivors network report, 1998). By United Nations estimates, there are more than 100 million uncleared mines worldwide (Korver, 1993). However many sources now consider this number to be overestimated (Cameron, 1998).
In our study, all footwear tests against AP landmines resulted in severe injuries to the lower extremity. Differing degrees of injury severity can result in different medical outcomes and this injury reduction is the area affected by current footwear.
The Wellco OB demonstrated a trend of marginal improvement in protection against the smallest mine tested (M-14). This footwear combination allowed for the conversion of a possible transfemoral amputation to a definite transtibial amputation with some potential for a salvageable limb with undetermined function.
Instrumentation of the cadavers led to a better understanding of the explosive event and provided a method of mine output comparison. Significant correlation of force data to the predicted medical outcome has been established and will be addressed in Volume 3 of this report. The surgical incisions and stress risers created in the tibia by load cell implantation may also affect the resultant injury pattern.
Direct contact blast has a different mechanism of injury than that of blunt trauma and
thus AP mine injuries do not lend themselves to prediction using current automotive industry force-time data. However the do follow similar trends at a different magnitude and this correlation will be further explored in Volume 3 of this report.
The cadaver model combined with the MTS offers the most reproducible biofidelic model currently available to scientifically study the AP mine injury to the lower extremities.
Based on sample sizes of 1 or 2 we found the following trends in our study:
- The Wellco blast boot alone probably offers no better protection than the standard CB alone.
- The BFR boot alone probably offers no better protection than the standard CB alone.
- The Med-Eng boot, which uses a different protection design, demonstrated some potential improvement in protection against the larger mines.
- When the Wellco OB is combined with inner protective (BB, BFR) footwear, there may be marginal additional protective effects against the medium and large mines when compared to the OB/CB combination.
Surgical management of blast mine injury is determined by the extent of injury to the bony and soft tissue structures. The soft tissue injury is often the most important of these factors, the amputative level being determined by the level at which, following debridement of dead and contaminated soft tissue, it is anticipated that there will be an adequate myoplastic flap and skin coverage for delayed primary closure. Amputation level will ultimately determine the degree of function for the landmine victim.
There is undoubtedly some difficulty and uncertainty in determining the level of tissue viability in the cadaver model. Whereas the level to which contamination extends can be relatively easily determined, the extent of the non-viable tissue from the blast injury is more uncertain. Except for gross tissue disruption, none of the clinically significant tests of tissue viability can be applied to the cadaver model.
The MTS value was assigned to each test cadaver by one of two experienced Board- certified military Orthopaedic Traumatologists, each of whom has a domestic practice consisting entirely of orthopaedic trauma. One surgeon gained field experience during the armed conflicts in Somalia and Haiti, the other in Bosnia and in treating Gulf War casualties. For the purposes of MTS evaluation, the surgeon was blinded to both the nature of footwear and the mine type in each case. Determination of the MTS value was done predominantly by inspection and dissection of the tissues; similar to the way it would be performed at initial surgery in the field. Post-test radiographs and computerized axial tomographs (CT scans) were also available for review during this process. In each case, the dissection was videotaped. An UK-trained Orthopaedic Surgeon who independently assigned MTS values reviewed the videotaped dissections. This surgeon gained extensive experience while engaged in humanitarian surgical programs treating landmine injuries in Afghanistan, Cambodia, Angola, Rwanda, and Sri Lanka.
Fractures occurring at the cemented interface between the load cell and tibia were regarded as artifacts (occurring due to the presence of a stress riser at this point) and not taken into account in the MTS scoring. Furthermore, when surgical closure failure at the instrumentation site occurred, it was not graded as an open injury unless wound propagation was noted.
Compared to other war injuries, landmine victims have been shown to require more operations (5.1 compared to 2.2) and a longer hospital stay (37.3 days versus 10) (Korver, 1993). Reduction in injury severity as a result from protective equipment may reduce the number of operations needed.
Patients requiring amputations (80% mine injured) require far greater volumes of post-operative blood transfusion than other war-injured patients. Korver (1993) reported that the requirements of the non-amputated group were 29.2 units of blood per 100 patients compared to 354 units of blood for the amputated group. This difference is even more significant when viewed in the context of third-world mine-affected countries where blood supplies are scarce and storage facilities limited. Reduction in the severity of injury as exemplified by the protection provided by the over boot against the M-14 mine may reduce the demand for transfusion.
In mine-affected countries, the large numbers of amputees have led to a massive demand for prostheses. For example, in Cambodia the incidence of amputees is 1 of every 236 persons in the population (Chaloner, 1996). Despite initiatives by governmental and NGOs to train native people to produce prostheses using locally available materials, the demand still far exceeds supply. Replacement prosthesis is needed every 3-5 years in an adult and every six months for a child, and so this increased demand will persist for many decades. In four of our test cases the injury to a foot protected by an over boot was thought not to require amputation (MTS 1 or 1A). Clinical cases with this pattern of injury would possibly avoid the need for prosthetic replacement.
Most of the countries with significant mine problems are third-world nations with agriculturally based economies. In the absence of prostheses, amputees are often deprived of their means of subsistence, becoming an economic burden on their families and communities. Where prostheses are available, there is a considerable functional difference between transfemoral and transtibial amputees. Through-knee amputations are seldom undertaken as they present very great difficulties for prosthetic production and fitting. It has been shown that transfemoral amputees are considerably less mobile, make less use of their prostheses, and have greater metabolic requirements in order to mobilize than transtibial subjects. With prostheses, the energy expenditure in a young amputee is 25% over baseline for a transtibial amputation, 40% for bilateral transtibial amputations, 65% for a transfemoral amputation, and 150% for bilateral transfemoral amputations. In victims who do not receive prosthesis, the energy requirements are increased 32% over the normal baseline of walking for a transtibial amputation victim with a three-point gait (Walters, 1987). Failure to consider the increased energy requirements for amputees explains why patients discontinue walking despite the availability of prosthetic care. Therefore, from a surgical perspective every attempt should be made to preserve the knee joint if possible. Preservation of the limb or an amputation that spares the knee joint carries many physiological advantages. Transtibial amputations in young people can have near normal function in certain activities of daily living with a minimal increase in the energy expenditure.
The International Committee of the Red Cross (ICRC) regularly deploys surgical teams to war zones around the world where the indigenous healthcare infrastructure is unable to cope with the numbers of injured or has collapsed because of the conflict. As such, the ICRC has extensive experience in the treatment of war-injured patients, including those injured by landmines, and has meticulous records of greater than 26,000 total cases.
Clinical experience and analysis of the ICRC data has led to the classification of landmine injury into three groups. (Coupland, 1991)
- Type I: Blast injuries to the lower body: This type of injury is the most common and is sustained from stepping on a buried blast mine, resulting in an amputation of the triggering limb, either above or below the knee. Mud, footwear debris, vegetation, and mine fragments are driven proximally in the limb, spreading along fascial and soft tissue planes. Contralateral limb soft tissue damage is often associated with this type of injury and the extent of damage is directly related to the relative size of the mine’s explosive charge. Injury to the perineum (groin) has been seen i
n larger mine blasts. - Type II: Fragmentation injury: This injury results from triggering a fragmentation mine or being in proximity to a blast mine explosion. This pattern involves multiple fragment wounds, most of which will be concentrated in the lower limbs but also may involve the abdomen and thorax.
- Type III: Detonations of a blast mine in proximity to the face, body, and hands: This injury arises from the detonation of a blast mine in proximity to the hand or face. It typically occurs when the victim is handling a mine or when a mine clearance worker inadvertently detonates a buried blast mine by probing it while in the prone or squatting position. This pattern of injury involves partial amputation of the upper limb(s) and blast/fragmentation wounds to the face, neck, and trunk. Each pattern of injury has its own type of specific mortality and morbidity in terms of sepsis, blood transfusion requirements, prosthetic needs, and rehabilitation concerns.
Several scoring systems exist which attempt to classify the extent and severity of war injury or severe injury to the limbs. Recognizing that scoring systems relating to peacetime injuries are not applicable to war wounds, the ICRC has developed its own wound scoring system. Although this system has been well received and widely used, Coupland in 1992 notes that a traumatic amputation resulting from a landmine cannot be scored easily by this system (Coupland, 1992 & Bowyer, 1993).
- Categories: Designed for quick and easy use in the field, this system assigns scores to each of 6 categories:
- E (Entry wound)
- X (Exit wound)
- C (Presence or absence of a wound cavity)
- F (Fracture characteristics, if present)
- V (Injury to a vital structure)
- M (Presence or absence of metallic foreign bodies in the wound)
- Grades: By evaluating each category and combing the scores, the war wound can then be graded as 1-3:
- Grade 1: Represents only minimal tissue damage.
- Grade 2: Represents significant tissue damage or comminuted fracture.
- Grade 3: The most severe of penetrating wounds.
Numerous clinical studies have been performed to devise classification systems relating medical outcome to severe limb injury. The purpose of most of these studies was to develop predictive indices that can assist a surgeon’s evaluation of the injured limb based on the degree of skeletal and soft tissue injury, the presence or absence of limb ischemia, and the presence of a hypovolemic state, in his decision to salvage versus amputate the severely injured limb. Several authors have described different scoring systems for severely damaged extremities such as the Mangled Extremity Severity Score (MESS) (Johansen, 1990), Mangled Extremity Syndrome Index (MESI) (Gregory, 1985); Nerve, Ischemia, Soft tissue, Skeletal, Age (NISSA) (McNamara, 1994); and others. However, these systems are based on retrospective data from civilian trauma centers and rely on the assessment of physiologic parameters such as blood pressure and the integrity of the nerve and vascular structures to determine if amputation or salvage is indicated.
None of the mangled extremity scores have been validated outside the originating institution. Based on retrospective data, the scoring systems do not define the injury and are often too complex. They are difficult to apply in the clinical setting, and do not address the issue of eventual function of the amputated or salvaged limbs, nor do they consider the impact of differing levels of amputation. It must be recognized that an amputated limb does not necessarily represent a surgical failure as the function with prosthesis may exceed that of the salvaged limb even after extensive reconstructive surgery. Furthermore, these scores rely on assessment of physiological parameters and are thus inappropriate to a cadaver model of landmine injury. The MTS predicts the possible clinical outcome for each of the types of footwear and mines tested in the cadaver model.
In view of the above extremity scoring system’s weaknesses, there is a need to develop a severity scale for landmine blast injury. This system should be based on the anatomic assessment of severity to define the injury. In our study the MTS is introduced as a method of evaluating the extent of injury, offering prognostic medical diagnosis and predicting the type of surgical intervention required. It also correlates the predicted medical outcomes to the level of protection provided by various types footwear against different mine threats. The MTS scores were assigned via surgical dissection of the injured limb in conjunction with radiographic views of the post-test specimen. In this regard the findings from the surgical dissection were by far the most useful and predictive for MTS purposes. Plain X-rays had little bearing on the MTS values other than in one case with a non-reconstructable severely comminuted intercondylar femor fracture requiring transfemoral amputation. The situation is similar to the surgical treatment of landmine victims in the field where, if faced with large numbers of injured patients, radiographs are unlikely to alter the initial operative plan for those wounds that obviously require amputation (Coupland, 1993). CT scans were similarly found to have little bearing on MTS scoring but did accurately determine the extent of periarticular fractures and are predicted to be useful in the development of a mathematical model of landmine injury. MRI was included in the pilot study to define the extent of soft tissue damage. However, this imaging study did not prove to be worthwhile. MRI relies on physiologic changes in fluid content to define the zone of injury. In the cadaver model, these changes did not occur and therefore resolution was poor. As a result, MRI scanning was discontinued as part of the experimental protocol after the pilot study.
Experimental Models for Landmine Injury: In order to assess the potential benefits of mine protective footwear a suitable test model is needed to simulate the injury pattern.
Although live and cadaveric animal models have been utilized to study other aspects of ballistic and penetrating injury (Bowyer, 1996) these are of limited use when investigating blast mine protection or injury because there is no animal model equivalent in complexity to the anatomy of the human foot, with or without footwear.
Surrogates of the lower extremity remain at a preliminary state of development (Hybrid II, THOR, FSL) and need to be validated against a more biofidelic model before widespread application. Many of these manikins were developed by the motor vehicle industry (United States Army Aeromedical Research Laboratory, 1997) and are designed to mimic human injury patterns from frontal impacts. These surrogates have been adapted for use in the absence of any injury criteria relating to blast injury to the lower limb. The parameters used to determine the risk of long bone fracture were taken from automotive crash testing data, but requires validation before manikins can be used in antipersonnel mine testing.
Similarly, mathematical models of landmine injury using finite element analysis (FEA) are in the embryonic state of development and in need of input from experimentally derived biomechanical data to accurately simulate the injury process.
Currently the best model for antipersonnel landmine injury is whole-body human cadaver testing. As single limb and partial body models lack accurate mass and movement, this limits their use for precise reproduction of the injury. While full body cadaver testing represents the closest available model for blast injury research, it is recognized that there is some loss of biofidelity in modeling soft tissue and neurovascular response.
The model adopted for cadaver instrumentation was based on those used in automotive crash testing (
Walters, 1976), with a combination of a load cell and strain gauges. Clinical experience dictated that diaphyseal long bone fracture was unlikely to be seen in the axial-loading of landmine injury. However, it was hoped that the instrumentation data would lead to an objective estimation of the quantity of blast attenuation provided by each type of footwear. The load cell data showed minimal differences with regard to peak load and loading rates for any of the footwear types or for the different types of mine. In most cases, the peak tibial load occurred in the first 2 milliseconds with a possible trend towards slower subsequent decay of the measured load with the blast attenuating footwear. Disruption of the combat boot sole with subsequent destruction of the soft and bony tissue possibly leads to a faster decay of the axially transmitted load. In contrast, the protective boots attenuate a large amount of blast energy protecting the sole of the inner boot, which remains largely intact, especially for the smaller mines, and thus acts as a force plate prolonging the transmission of this load.
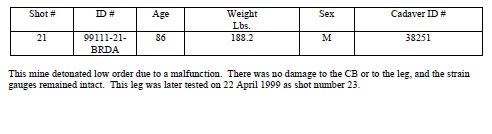
Consistency of the load cell data offered a degree of quality assurance with regard to each explosive event. For example, test 21 was a “low order” mine detonation, a recognized and occasional anomaly of explosive detonation in which the some of the charge fails to initiate. This was evidenced not only by lumps of residual explosive both within and around the mine but also by the load cell data where the characteristic peak was absent. In each of the other test cases, the characteristic peak loads were noted, suggesting that no further low order detonations occurred.
In the pilot study, strain gauges were placed on the distal femur. Realizing that strain failure was not occurring in the long bones and that there were no differences between the time to peak strain or peak strain for the various types of footwear, the gauges were moved distally to distal tibia and calcaneus where bone failure occurred. It was hoped that this instrumentation would deliver “strain to failure” data for these bones. However, the instrumentation was almost uniformly disrupted by the explosive event.
When resultant peak load data is plotted against time to peak load for the various MTS scores (Figure: 17) there does not appear to be a correlation. Superimposed on the same figure are injury predictive curves for long bone failure in axial loading of the lower limb derived from automotive crash testing (United States Army Aeromedical Research Laboratory, 1997). MTS values denoting severe injury fell below the low risk threshold curves invalidating the use of existing automotive crash test risk curves in predicting direct contact mine injury.
 (Mertz, 1993)")
Figure 17: MTS to Femur Injury Threshold Curves (Hybrid III) (Mertz, 1993)
The detonation of a blast mine is composed of several events. These begin with a single positive pulse that radiates from the source with a velocity in air approximately 1500 m/s, a negative phase, and then a mass movement of air behind the shock front with very high velocity and pressure, known as the dynamic overpressure. The measured rise time and duration of the force pulses roughly correspond to those reported for detonations of TNT.
When the shock wave encounters a solid surface, such as a boot sole, some of the energy will be absorbed and some transmitted. If the amount absorbed exceeds a critical level, the surface will fail, leading to the direct transmission of blast to the foot. In the absence of any blast-absorbing material most of the absorbed energy will be transmitted through the boot sole and into the tissues of the foot. The relative acceleration of the tissues will lead to stretching and tearing. Rapid multidirectional loading of the bones of the foot can cause fractures. As the blast wave continues to propagate, the injury spreads proximally, particularly following fascial planes, which represent the line of least resistance. If the sole of the boot is breached then there will be secondary blast injury due to fragments of soil, landmine and footwear, becoming embedded in the tissues.
For the purposes of this study, it was assumed that there was little variation in explosive profile between mines of the same type. The force generated by the detonation of an explosive is dependent on the type of explosive, weight, shape, and the density with which it is packed. Most of these parameters can be assumed the same for each mine type. There may be some variation in the explosive profile depending upon the “ shelf life” and explosive storage conditions for the individual mines. Good quality control of U.S. manufactured mines can be assumed; however, the same cannot necessarily be said for foreign mines.
In those cases where the hind foot and ankle were not completely disrupted, we detected a distinct pattern of anatomical injury. Typically, there would be a longitudinal skin laceration over the plantar surface of the foot, often associated with tangential lacerations over the medial side of the ankle. The incision for strain gauge instrumentation was performed on the lateral side of the hind foot and ankle. This wound was, in many cases, extended distally along the lateral border of the foot by the mine injury. On deep dissection, a characteristic pattern of bony failure was noted. This would typically involve a comminuted calcaneal fracture, fracture of the dome of the talus extending from anteromedial to posterolateral, and a pilon fracture of the ankle. Associated fractures were to the navicular and talar neck.
In order to be effective in preventing injury, mine protective footwear has to reduce the amount of energy transferred to the tissues of the foot. Design philosophy for this centers around four strategies. The first is standoff, where the bearing platform is distanced from the explosive. As blast energy transmission will attenuate in air according to the cube root of the propagation distance, so the amount of energy impacting the sole of the foot will be reduced. Where standoff is achieved only through increased sole thickness, there is still direct contact; energy transfer and energy transmission will not be reduced as effectively. The second involves blast attenuation, utilizing materials in the construction of the sole whose physical properties are altered during the explosive event. This allows the blast energy transmission to be reduced through the work needed to alter the footwear’s physical properties. The third strategy involves blast deflection, where an angled plate or the angled design of the sole is used to redirect the blast wave away from the foot. However, in real world application, foot location or plate orientation can vary, resulting in a plate orientation that increases energy transmission. For example, a 45°-midline angle that possibly deflects blast energy for a centerline mine detonation could potentially become a flat plate due to a side of the boot detonation. The fourth method is off-axis detonation, where the mine is detonated at some distance out away from the foot, which allows the bulk of the blast energy to bypass the limb.
The Wellco over boot appeared to mitigate the effects of M-14 landmine injury. This boot utilizes both standoff and blast attenuation as design factors. Standoff is achieved by virtue of a combination of the height of the over boot and inner boot soles, which increases the distance between the point of mine detonation and the sole of the foot. The aluminum honeycomb attenuator in combination with the Kevlar Aramid insole provides blast attenuation. A V-shaped deflective device positioned in the heel and instep areas is also utilized for blast deflection. The boot upper is also lined with two layers of Kevlar. On inspecti
on of the fast frame photography it appears that the boot acts by a decoupling mechanism, by “peeling off” the inner boot as the explosive event progresses. There may be a slight trend towards improved MTS scores (from 3 to 2B) when the over boot is used in combination with another blast protective boot rather than the standard combat boot for the larger mines. Furthermore, gross inspection of the inner boot (appendix D) would suggest a lesser degree of disruption of blast protective inner boots when compared to the standard combat boot.
Conclusions
The results of our study suggest some improvement in MTS with the use of the over boot when confronted with the smallest mine, the M-14, containing only 28 g of explosive. (Figure 3). The level of potential improvement is approximately one point on the MTS, converting a “3” injury (transtibial amputation and possibly transfemoral) to an injury defined by a mean MTS of between 1B and 2, a transtibial amputation but with the possibility of limb salvage. Although the LEAP study tested different types of footwear, sufficient tests to reach meaningful conclusions were conducted only for the over boots in comparison to the standard combat boot. Limited testing was done on other types of anti-mine protective footwear. These included the blast protective combat boot, the BFR boot, and the Med-Eng boot.
The Wellco® Blast Boot and the BFR boot, based on only one and two tests, respectively, both resulted in a severe spectrum of injury (2B’s and 3’s) when subjected to the smallest test mine, the M-14 (figure 3). Given limited experimental resources and the severity of injury produced with even the smallest test mine, no further tests using these boots alone were conducted. There remains the potential that some demonstrable benefit could be seen by using these boots, with more extensive testing. Based on the limited tests conducted, the study team concluded that these boots were unlikely to offer any greatly increased protection when compared to the standard combat boot.
The Med-Eng boot utilizes differing design principles than the other footwear tested and was the boot that that showed the most promise against medium and larger size mines. The boot was tested in two configurations; two tests (in the manner for which designed) with the PMN mine under the pod and one test with the PMA-2 mine on the center of the boot midline. The PMN tests both resulted in closed injury with MTS scores of 1 and 2A, respectively, and the PMA-2 test in an injury of MTS 2A (Figures, 4 & 5).
Until recently, sandals have been a common form of footwear used by deminers around the world. There have even been largely anecdotal reports suggesting that by early failure of the footwear and lower extremity with minimal secondary wound fragment damage; this may produce a less severe spectrum of injury than more substantial footwear (Traverso, 1981). During the Vietnam conflict, there was a common belief that wearing footwear and stepping on a landmine would result in a more severe injury compared to the bare foot. For comparison two tests were performed, using improvised sandals. These tests resulted in an MTS of 2B for an M-14 mine and an MTS of 4 for a PMN mine. From these tests, it appears that the spectrum of injury when wearing sandals is approximately equal to that of the combat boot (Figures, 3 & 5).
Several tests with over boots produced closed injuries (MTS 1 or 2), however even the closed injuries all feature various degrees of severe hind foot and ankle injury with any combination of calcaneal, talar, or tibial pilon fractures. While a closed injury avoids the gross contamination and potential septic sequelae of a standard mine injury, the eventual functional outcome of such severe hind foot bony disruption may be no better than a transtibial amputation. The fact that the MTS does not address the eventual functional outcome of these closed injuries represents a weakness in the scoring system.
In countries experiencing landmine casualties, comparison of functional outcomes is dependent on local factors beyond the mere extent of the injury. Medical supplies and the availability of open reduction and internal fixation resources for the hind foot fractures and prosthetic provision for the amputees will determine the treatment options in third-world countries. While no specific reference exists regarding the likely outcome of these closed, severe, mid foot, and/or hind foot fractures, it is reasonable to conclude that overall function is likely to be poor. A stiff, painless ankle and foot may act as a biologic prosthesis, however limbs with severe pain may require an ankle and /or subtalar arthrodesis. The ability to perform open reduction and internal fixation of these hind foot fractures is rarely available in a third-world setting.
With reference to the ICRC data and publications relating to mine injuries, it is possible to draw conclusions with regard to the nature of injuries seen in the LEAP study test cases. In ICRC hospitals mortality from landmine injury is 3.5% (Eshaya-Chauvin, 1992). However, it is well recognized that this is an underestimate of the true overall mortality, as many cases will die at the point of wounding or during the prolonged evacuation times necessary to reach a surgical facility. In approximately 30% of cases, this evacuation time is over 24 hours (Coupland, 1991).
Similar to other war wounds, landmine injuries are grossly contaminated with mud, vegetation, mine casing, and footwear debris. Initial surgery with wound debridement and excision is designed to reduce the burden of this contamination and when combined with postoperative antibiotics to prevent sepsis. Despite these measures, in ICRC hospitals postoperative fever is seen in around 50% of amputees (mostly mine victims) once malaria has been excluded (Korver, 1993). The conversion of an open injury with contamination to a contained or even a closed injury should decrease the risk of infection and allow the extent of surgical resection to remain a transtibial amputation. The LEAP study demonstrated that use of the over boot against the smaller AP mines may result in closed injury or in a contained injury, without the gross contamination typically associated with landmines. As such, the burden of septic complications may be reduced.
Recommendations
- The Med-Eng boot demonstrated potential improvement in protection against the larger mines and additional testing of this type of footwear is warranted.
- Over the period of this study, several nations (United Kingdom, Canada, Russia) have developed mine protective footwear. Each employs various types of protective materials, standoff distance, and trigger mechanisms. An evaluation of this new footwear using the testing methodology developed in this study is recommended.
- Cadaveric testing is the most biofidelic model to accurately define the level of potential protection of any footwear. This method gives a reproducible, cost-effective test method for AP mine injury assessment and should be utilized in future protocols.
- Due to the possibility of variability in live mine detonation, a mine surrogate utilizing cast and pressed TNT (based on threat mine prevalence) will give the best repeatable blast profile.
- Our model evaluated the footwear only without the Kevlar pants. Additional testing is required to determine if there is any benefit or detriment to the lower extremity with the use of the P3I suit.
- The P3I countermine suit requires further testing to define the limitations of the equipment and to evaluate its ability to protect against Type II and III landmine injuries.
- The effects of secondary missiles from the metal attenuators or other boot materials warrant evaluation with further testing on whole body cadavers.
- No further testing is necessary for the BB and BFR boots alone.
References
- Banks E., (1997). Anti-personnel landmines: Recognizing and disarming. London: Brassey’s.
- Bowyer, G. W., Cooper, G. J., & Rice, P. (1996). Small fragment wounds: Biophysics and pathophysiology. The Journal of Trauma, 40 (3), S159-S164.
- Bowyer, G.W., Stewart, M. P. M., & Ryan, J. M., (1993). Gulf war wounds: application of the Red Cross wound classification. Injury, 24, 597-604.
- Cameron, M. A., Lawson R. J., & Tomlin, B.W. (Eds.) (1998). To walk without fear: The global movement to ban landmines. Toronto: Oxford University Press.
- Chaloner, E. J., & Mannion, S. J., (1996). Antipersonnel mines: the global epidemic. Annals of the Royal College of Surgeons of England, 78, 1-4.
- Coupland, R. M., (1993). Management Principles. In: War wounds of limbs: surgical management. Oxford: Butterworh-Heinemann.
- Coupland, R. M., (1992). The Red Cross classification of war wounds: The E.X.C.F.V.M. scoring system. World Journal of Surgery, 16, 910-917.
- Coupland, R. M., & Korver, A. J. H., (1991). Injuries from antipersonnel mines: the experience of the International Committee of the Red Cross. British Medical Journal, 303, 1509-1512.
- Croll M., (1998). The history of landmines. Barnsley, Great Britain: Pen & Sword Publications.
- Eshaya-Chauvin, B., & Coupland, R. M., (1992). Transfusion requirements for the management of war injured: the experience of the International Committee of the Red Cross. British Journal of Anesthesia, 68, 221-223.
- Garachon, A., (1993). ICRC rehabilitation programs on behalf of war disabled. In: Report of the Symposium on Anti-personnel mines. Montreux, Geneva: International Community of the Red Cross.
- Gray, B., Henningsen, M., Leeson, K., Maddocks, I., Poy, P. P., Teague, D., & Von der Borch, A., (1997). The landmine epidemic. In Landmines, a global health crisis: International Physicians for the Prevention of Nuclear War report number 2 (pp. 1-7). Cambridge: USA, International Physicians for the Prevention of Nuclear War
- Gregory, R. T., Gould, R. J., Peclet, M., Wagner, J. S., Gilbert, D. A., Wheeler, J. R., Synder, S. O., Gayle, R. G., & Schwab, W., (1985). The mangled extremity syndrome (MES): A severity grading system for multisystem injury of the extremity. Journal of Trauma, Injury, Infection and Critical Care, 25 (12), 1147-1150.
- International Humanitarian Law. (Version 5) [CD-ROM]. (1998). Geneva: International Committee of the Red Cross Publications [Producer and Distributor]
- Johansen, K., Daines, M., Howey, T., Helfet, D., & Hansan, Jr., S., (1990). Objective criteria accurately predict amputation following lower extremity trauma. Journal of Trauma, 30(5), 568-573.
- King, K. F., (1969). Orthopaedic aspects or war wounds in South Vietnam. Journal of Bone and Joint Surgery, 51(B), 112-117.
- Korver, A. J. H., (1993). Injuries of the lower limbs caused by antipersonnel landmines: the experience of the International Committee of the Red Cross. Injury, 24, 607-609.
- Landmine casualty data report: Deminer injuries. (2000, February). United States Department of Defense, Office of the Assistant Secretary of Defense for Special Operations / Low Intensity Conflict. Washington, DC:
- Landmine Survivors Network. (1998, July). Surviving the scourge of landmines. (Conference report). Amman, Jordan:
- McNamara, M. G., Heckman, J. D., & Corley, F. G., (1994). Severe open fractures of the lower extremity: a retrospective evaluation of the Mangled Extremity Severity Score. Journal of Orthopaedic Trauma, 8 (2), 81-87.
- Taylor, J. H. B., (1999, September). Blast mines study, (Available from CBD Porton Down Biomedical Sciences Division, England)
- The Technical Cooperation Program. (1998). Protection of soft-skinned vehicle occupants from landmine effects. (Technical Report, Technical Panel W-1, Key Technical Activity 1-29). Quebec, Canada: Defence Research Establishment Valcartier.
- Time-Life Books. (1998). The south’s infernal machines. In Time-Life Books’ Echoes of glory: Arms & equipment of the confederacy. (pp. 302-303). USA: Time Life Inc.
- Traverso L. W., & Fleming, M. C., (1981). Combat casualties in northern Thailand: Emphasis on land mine injuries and levels of amputation. Military Medicine, 146, 682-685.
- United States Army Aeromedical Research Laboratory (1997, July). Mine blast acceleration injury assessment: Methods, criteria and software. (USAARL Report No 97-28). Fort Rucker, Al: Alem, N. M.
- United States Army Yuma Proving Ground (1999, September). Final test report for the developmental test (DT) /operational test (OT) of the body armor set, individual countermine preplanned product development (Basic P3I). (YPG Document No. 99-015). Yuma Proving Ground Tropic Test Center, Panama: Tijerino, D., & Hay, L.
- Walters, R. L., Campbell, J., & Perry, J. (1987). Energy cost of three-point crutch ambulation in fracture patients. Journal of Orthopaedic Trauma, 1 (2), 170-173.
- Walters, R. L., Perry, J., Antonelli, E. E., & Hislop, H., (1976). Energy cost of walking of amputees: The influence of level of amputation. Journal of Bone and Joint Surgery, 58-A, 42-46.
Appendix A
Detailed Medical Evaluations
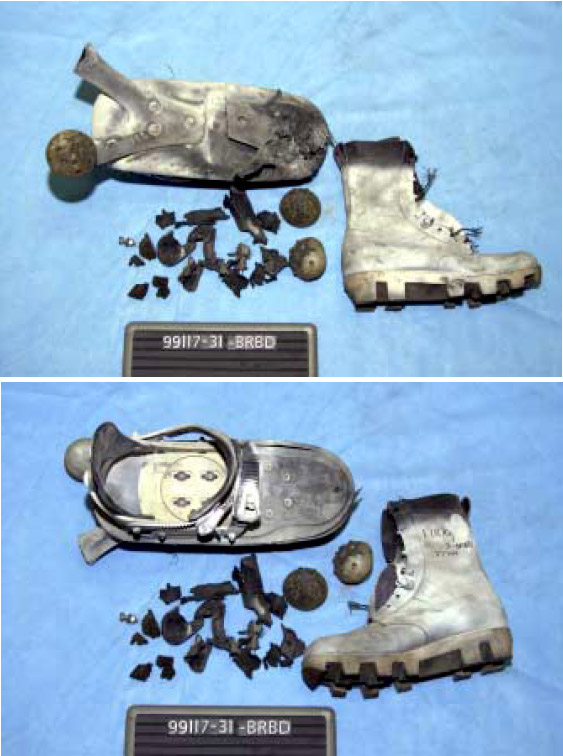
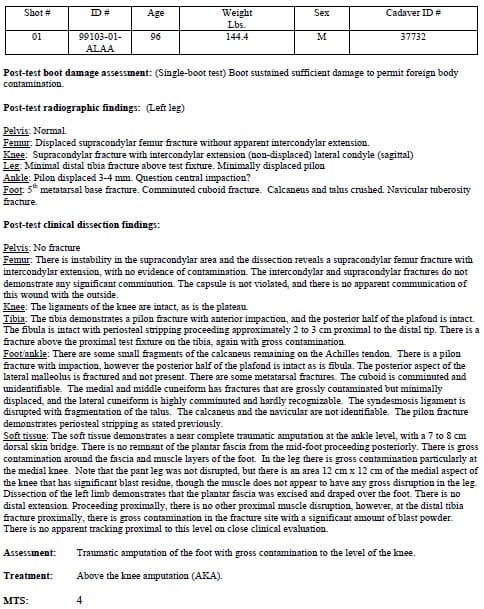
shot #1
shot #2
shot #3
shot #4
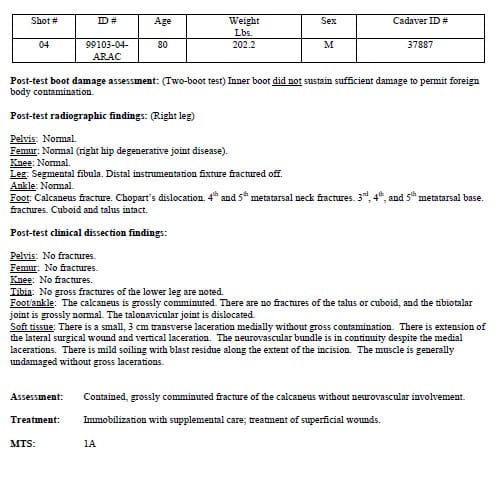
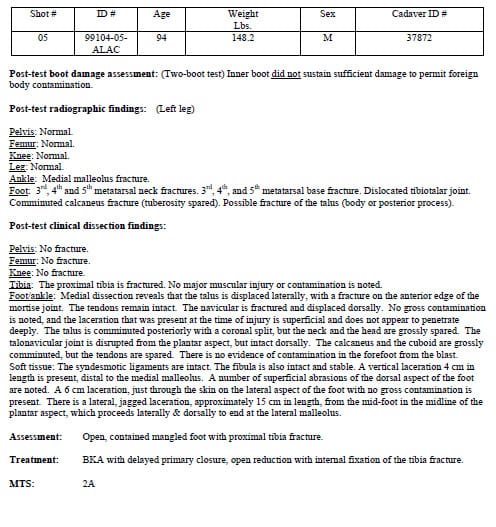
shot #5
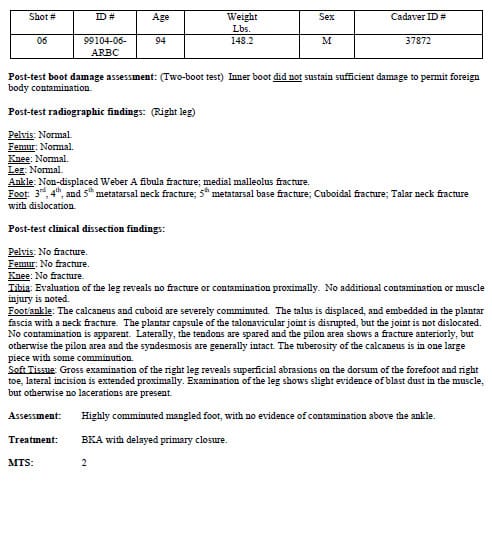
shot #6
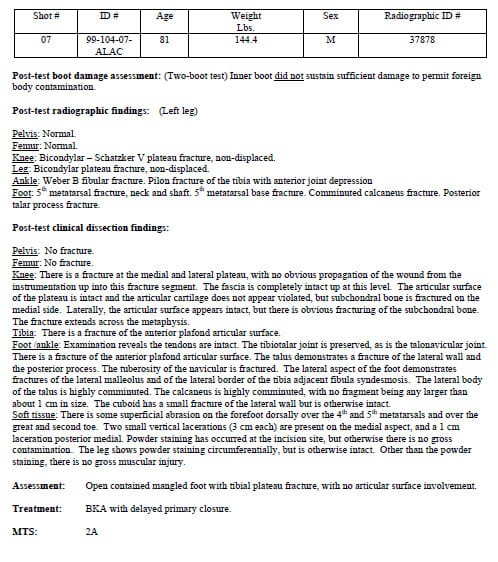
shot #7
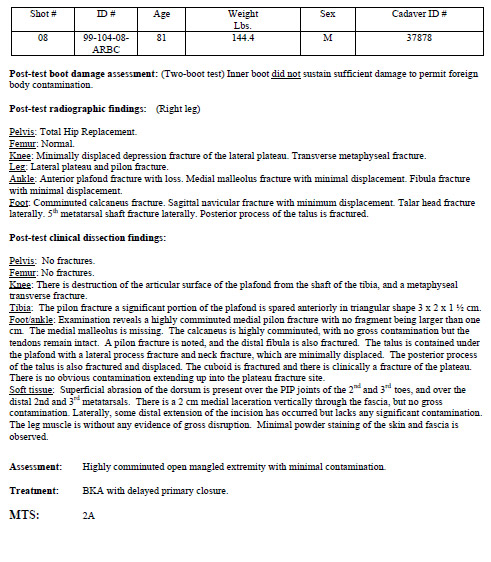
shot #8
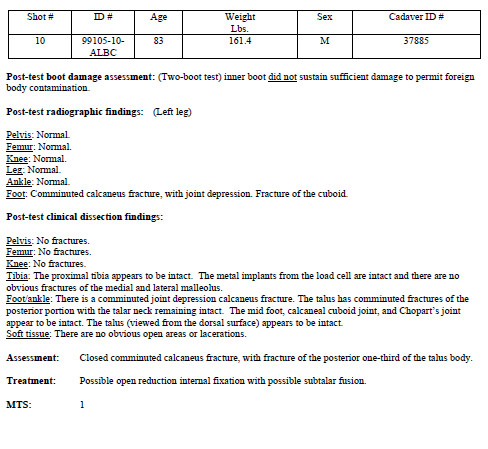
shot #10
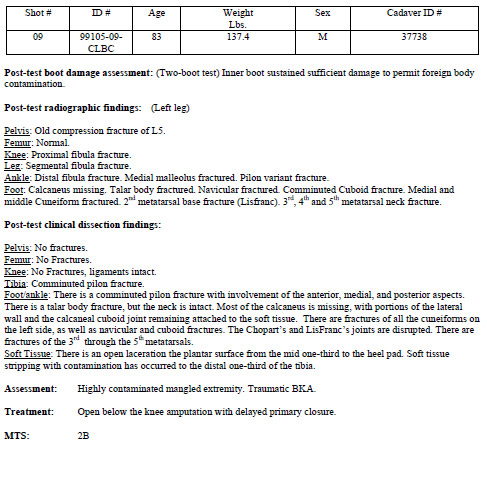
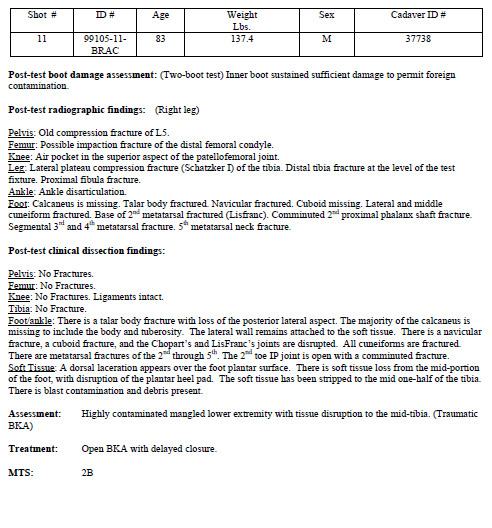
shot #11
shot #12

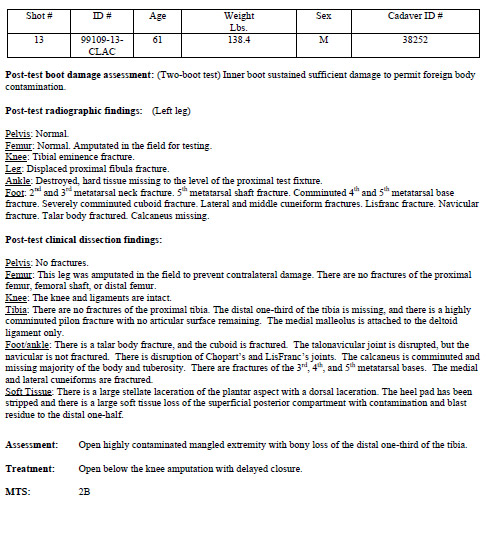
shot #13
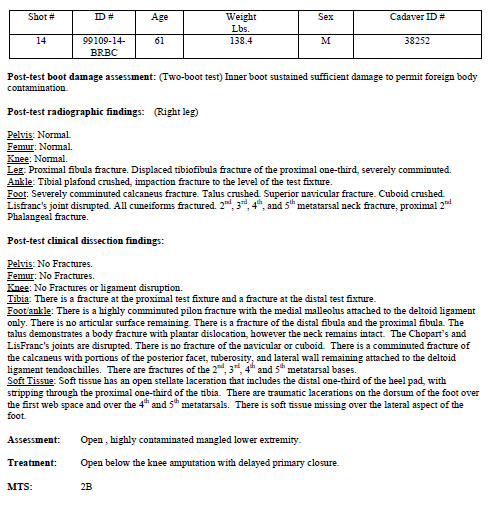
shot #14
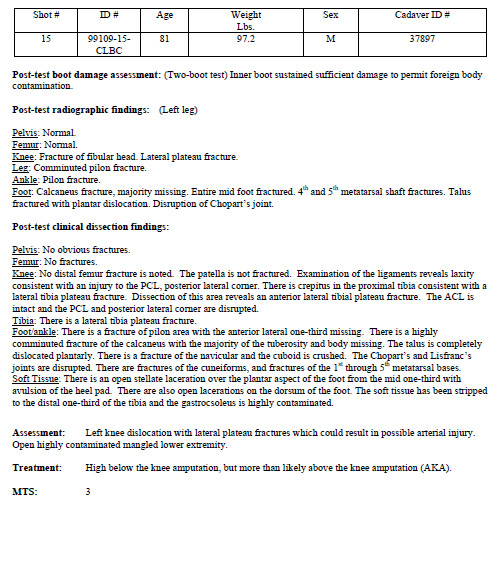
shot #15
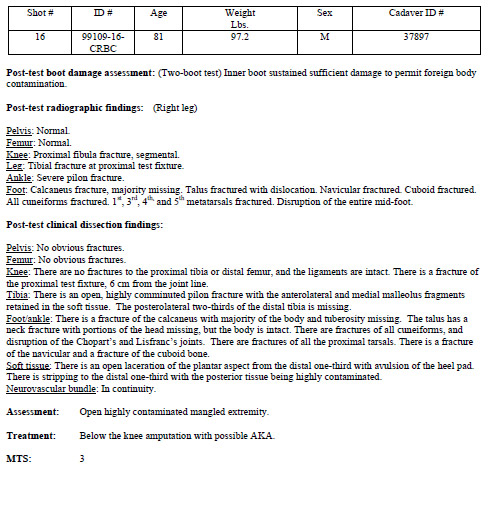
shot #16
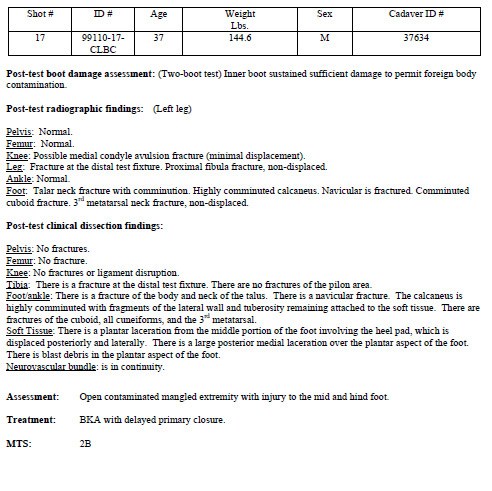
shot #17
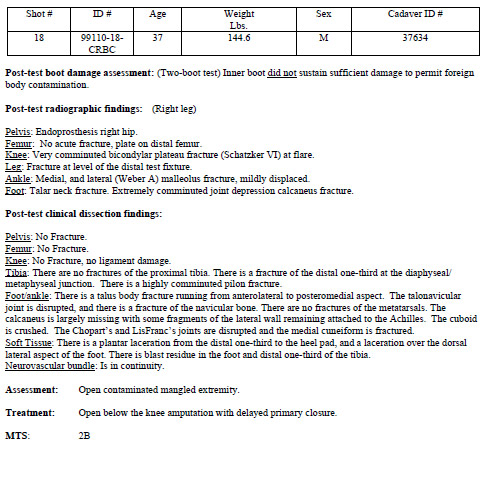
shot #18
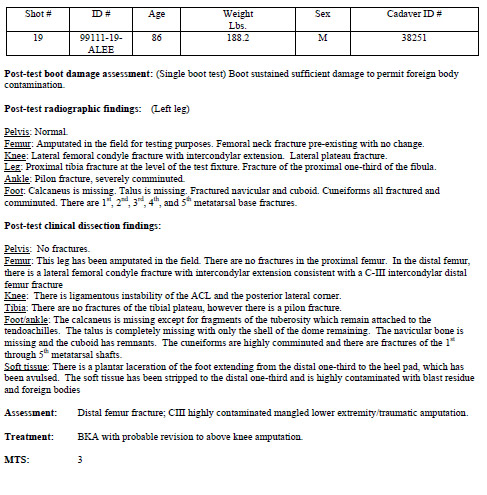
shot #19
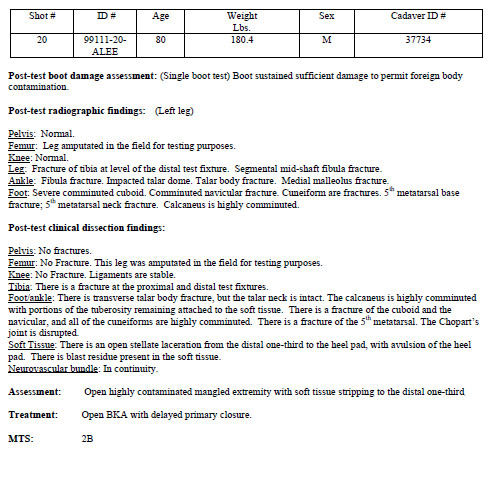
shot #20
shot #21
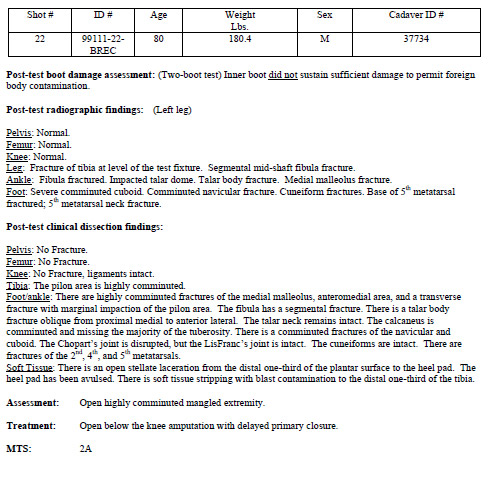
shot #22
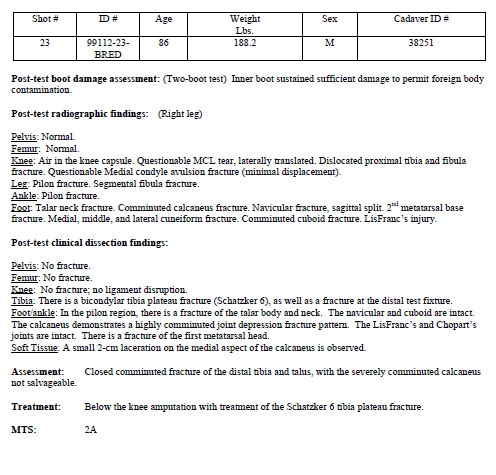
shot #23
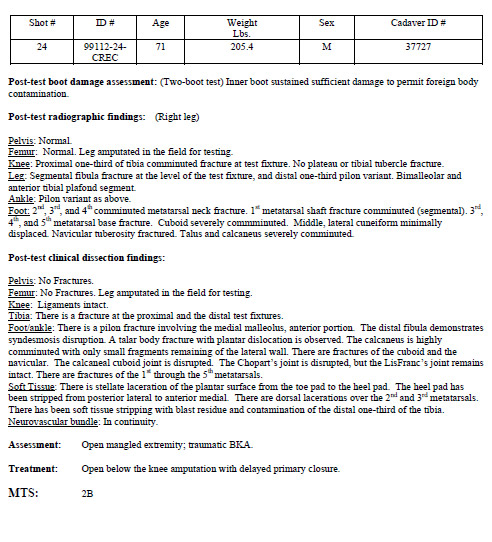
shot #24
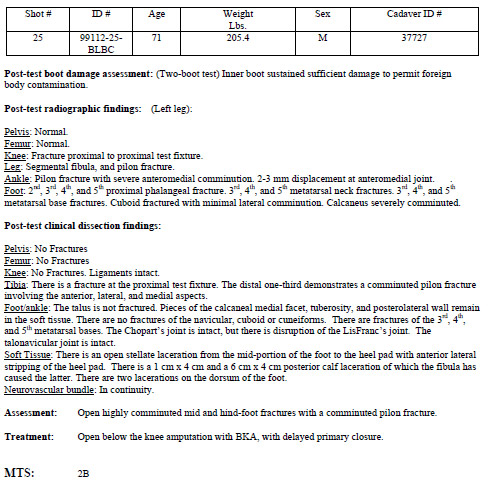
shot #25
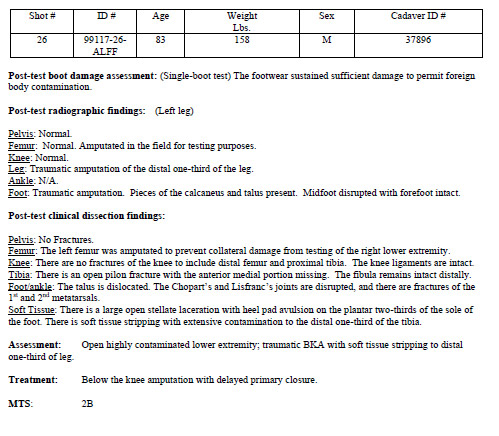
shot #26
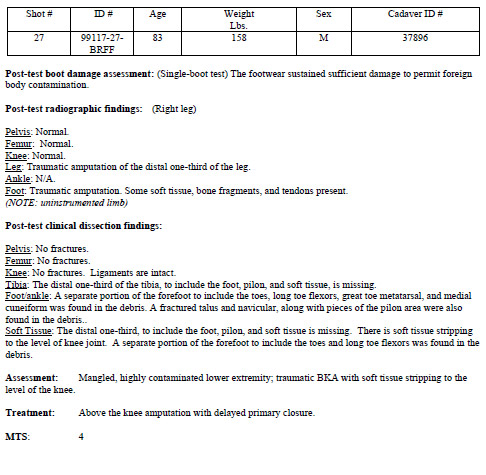
shot #27
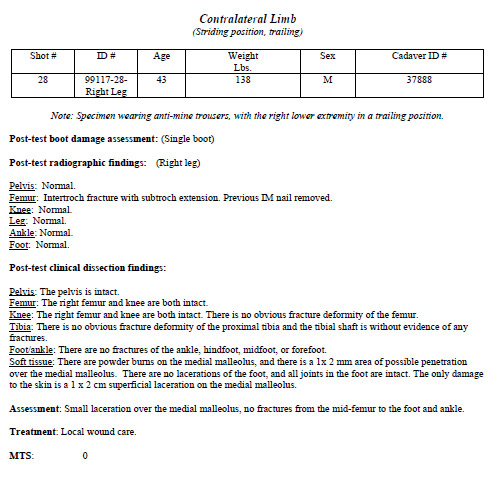
shot #28
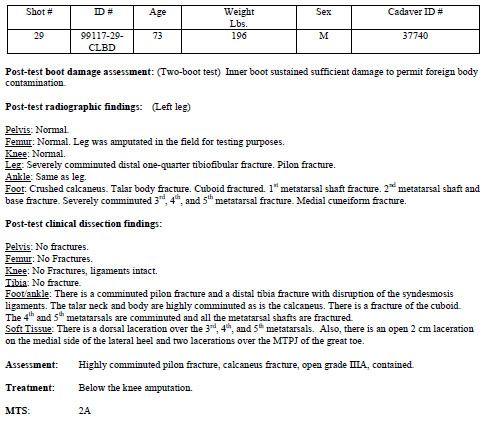
shot #29
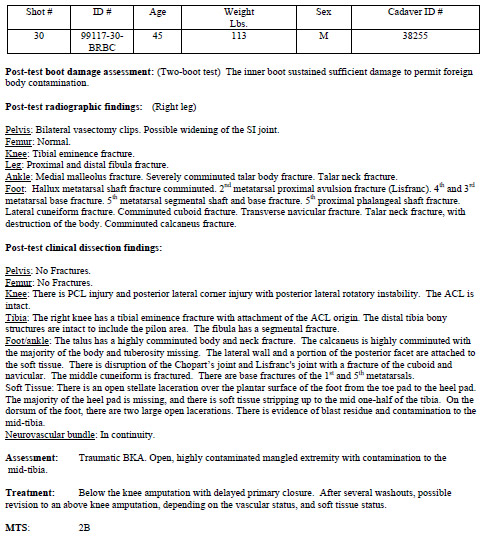
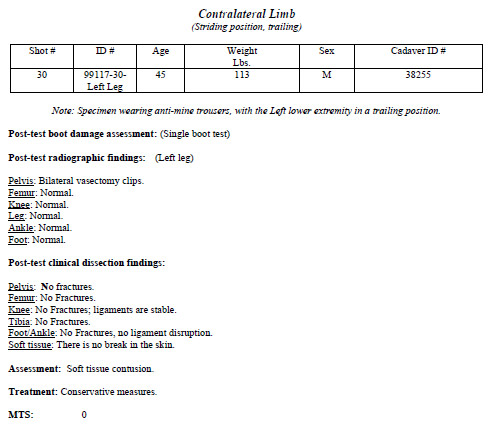
shot #30
shot #31
Appendix B
Pretest Radiographs
Pretest Radiographic Evaluations: The following pictures illustrate examples of the radiographic views utilized for the LEAP 99-2 study. These are examples of normal specimens taken before testing.

Picture 1AP Pelvis

Picture 2 AP Femur

Picture 3 Lateral Femur
Picture 4 AP Knee

Picture 5 Lateral Knee
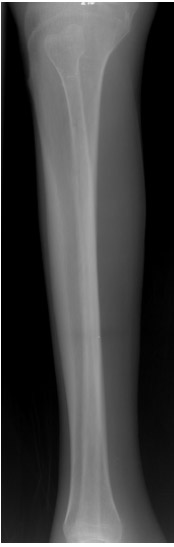
Picture 6 AP Leg

Picture 7 Lateral Leg

Picture 8 AP Ankle
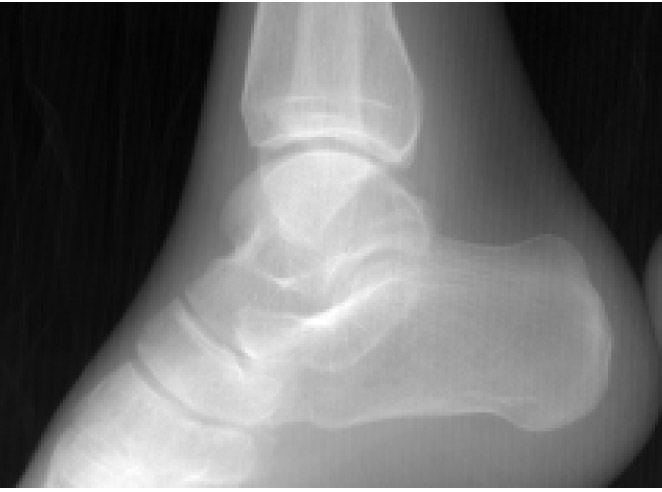
Picture 9 Lateral Ankle

Picture 10 AP Foot

Picture 11 Lateral Foot
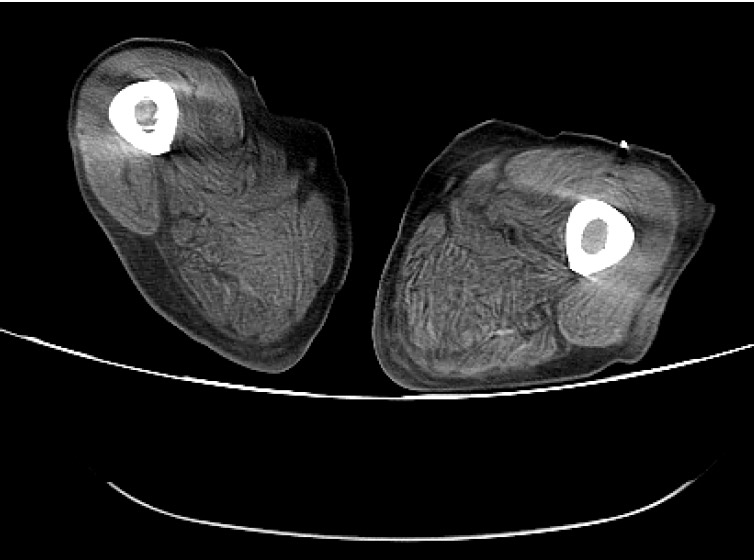
Picture 12 CT Femur
Appendix C
Post test Radiographs
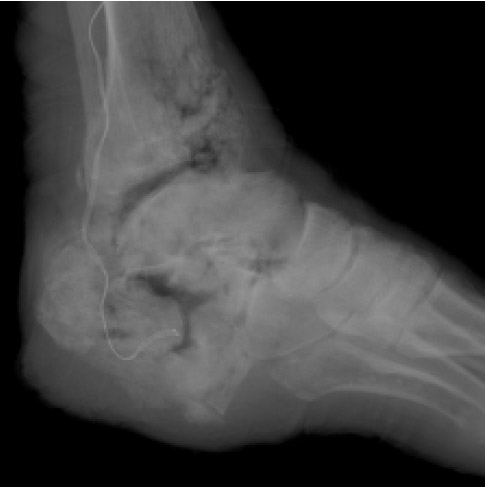
This appendix contains representative radiographic examples of each injury according to the Mine Trauma Score.

Picture 1 MTS 0

Picture 2 MTS 1

Picture 3 MTS 1A

Picture 4 MTS 1B No injuries of this type occurred during testing.
(Note: Picture 4 was not included in the Report)

Picture 5 MTS 2
Picture 6 MTS 2A

Picture 7 MTS 2B

Picture 8 MTS 3

Picture 9 MTS 4
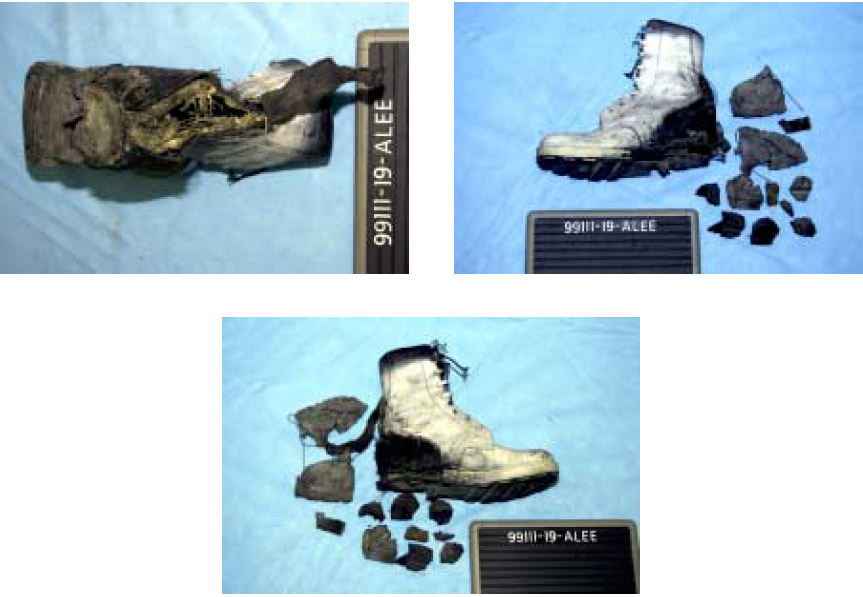
Shot # 19 ID # 99111-19-ALEE
M14 Mine with Singapore manufactured boot.
The rear 4 inches of the heel portion of the sole has been removed by the blast. The Kevlar insole is frayed around the edges and has a 1½-inch lateral tear at mid-heel and a longitudinal tear on the medial side of the heel penetrating the bottom layers of the material. The leather upper remains attached to the Kevlar insole. There is a 3-inch vertical tear in the leather upper, over the medial portion of the heel approximately 3 inches forward of the Achilles seam. A 6-inch vertical tear along the Achilles seam has penetrated the leather upper and the underlying Kevlar liner completely. The leather covering the heel cap portion of the boot has been completely separated from the upper exposing the Achilles seam.
Shot # 20 ID # 99111-20-ALEE
M-14 Mine with Singapore manufactured boot
The rear 4 inches of the heel portion of the sole has been removed by the blast and recovered in several large pieces. There is a 2-inch longitudinal tear in the lateral side of the sole at mid-foot. The leather upper has been completely separated from the sole and the Kevlar insole throughout the heel area. The leather heel cap portion of the upper has been badly shredded and completely separated from the boot. A vertical tear along the Achilles seam, which penetrates the leather upper and Kevlar lining, has opened the entire back of the boot. There is a 1-inch tear in the Kevlar lining at the rear of the heel.

Shot # 21 ID # 99111-21-BRDA
PMN mine with standard combat boot/Canadian overboot combination
(Note: This shot was low order due to a detonation malfunction.)
The left rear leg of the Canadian overboot has been removed by the blast. The area of the sole immediately above the left rear leg has received some damage and several cracks are vi
sible. The right rear leg has received some superficial damage and is missing its rubber pod; otherwise, the overboot appears to be intact and undamaged with no damage to the bindings/attachment plate.
The combat boot is intact and appears to be undamaged. Removal of the cushion insole reveals no damage to the leather insole of the combat boot.

Shot # 22 ID # 99111-22-BREC
PMN Mine with Singapore manufactured boot/overboot combination.
The heel portion of the overboot sole has been completely destroyed by the blast, and recovered in several large pieces. The blast deflector, attenuator, and attenuator plate were completely separated from the overboot. The blast deflector has been partially flattened and bent upward approximately one-half inch at its center. The attenuator remains attached to the attenuator plate and has been completely compressed throughout its length with several long strips shredded from each side. The attenuator and attenuator plate have been bent upward approximately ½ inch in the center and slightly twisted. The Kevlar insole remains attached to the overboot and appears to be intact and undamaged. The medial portion of the Kevlar upper remains attached to the Kevlar insole and is apparently undamaged. Approximately 5 inches of the lateral portion of the Kevlar upper has been separated from the heel area of the Kevlar insole, but is otherwise undamaged. Both sections of the Kevlar upper have been completely separated at the Achilles seam.
The sole of the Singapore blast boot is apparently undamaged. There is a 1 ½-inch vertical tear in the black cloth lining inside the boot 1 inch above the insole directly over the Achilles tendon. There are no tears or apparent damage to the leather upper of the boot, however the white paint applied to the boot pre-test has flaked off along wrinkle lines indicating there was some compression of the leather upper.

Shot # 23 ID # 99112-23-BRED
PMN mine with Singapore boot/Canadian overboot combination.
The Singapore manufactured blast boot used in this test is missing and not available for examination.
The rear two legs of the Canadian overboot were completely removed by the blast. Fragments of the legs were recovered along with one intact pod and one fragmented pod. A 1½ inch x 2 inch section at the extreme rear portion of the overboot has been destroyed. The screws attaching the rear set of legs to the overboot remain in place. The lateral edge of the insole plate of the overboot has sustained a 7-inch crack in the material from the heel to the mid-foot. There appears to be no damage to the bindings or binding attachment plate.
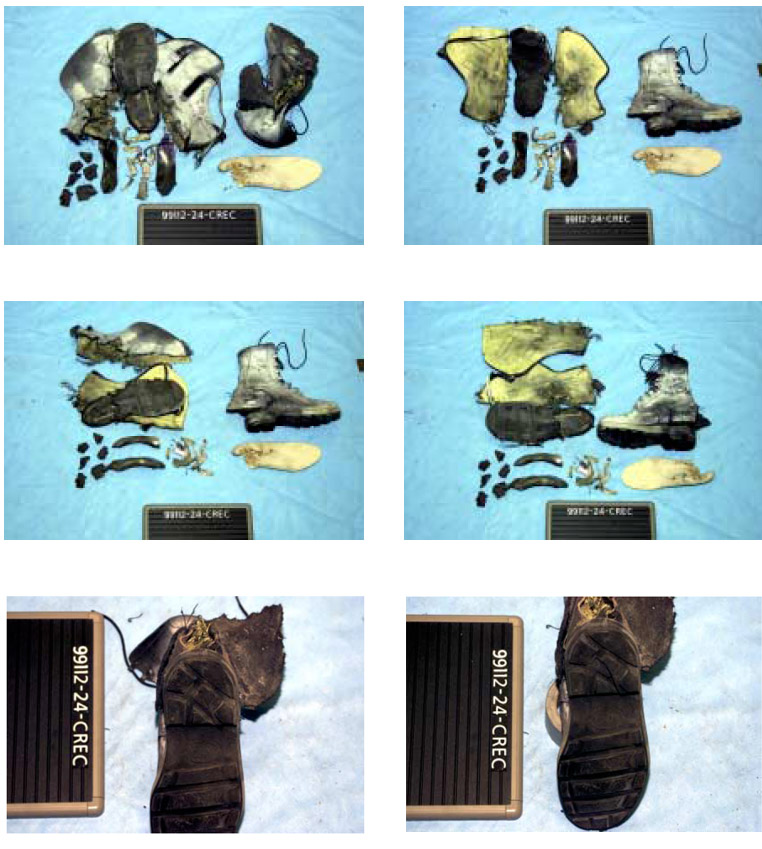
Shot # 24 ID # 99112-24-CREC
PMA-2 Mine with Singapore boot/overboot combination.
The rear 4 inches of the overboot sole has been completely destroyed by the blast. The blast deflector, attenuator, and attenuator plate have all been completely separated from the overboot. The blast deflector has been badly flattened and folded, resulting in a 3-inch split in the metal along the rear two-thirds of its mid-line. The blast deflector has also been bent upward approximately 1 inch in its center. The attenuator has been separated from the attenuator plate and shredded into several small fragments, which have been completely compressed. The attenuator plate is bent upward approximately 1 inch in its center. The Kevlar insole remains attached to the overboot, and appears to be undamaged. Its canvas cover remains attached, but has sustained several small tears over the midpoint of the heel. Both the medial and lateral portions of the Kevlar upper have been completely separated from the overboot, and have been separated down the Achilles seam. The medial portion of the Kevlar upper appears to be undamaged, while the lateral portion has a 3 ½-inch vertical tear with extensive shredding in the Kevlar material over the lateral portion of the heel 3 inches forward of the Achilles seam.
The sole of the Singapore boot has sustained a 2 ½-inch longitudinal tear over the mid-heel. The sole has been separated from the leather upper and insole of the boot from the heel to mid-foot. The Kevlar insole appears to be undamaged. There is a 6-inch vertical tear completely through the leather upper and Kevlar lining along the Achilles tendon. The Kevlar lining over the insole appears to be intact. The heel portion of the cushion insole has been badly shredded. The white paint applied pretest to the boot has flaked off along wrinkle lines indicating compression of the leather upper.
Shot # 25 ID # 99112-25-BLBC
PMN mine with blast boot/overboot combination
The rear 4 inches of the heel portion of the overboot has been destroyed and recovered in several large pieces. The blast deflector and attenuator have been separated from the overboot. The blast deflector has been moderately flattened, and bent upward approximately one-half inch in its center. The attenuator has been compressed and shredded down its entire length. The attenuator plate remains affixed to the underside of the Kevlar insole. The Kevlar insole remains attached to the overboot and appears to be intact and undamaged. Both sides of the Kevlar upper have been separated from the sole of the overboot from the heel to mid-foot. Both halves of the Kevlar upper have been completely separated at the Achilles seam, but there appears to be no damage to the Kevlar material itself. The blast deflector, attenuator, and attenuator plate of the blast boot have been flattened/compressed in the center causing the rear portion to tear through the sole of the blast boot in the heel area between the lugs of the sole. The blast deflector, attenuator, and attenuator plate remain attached to the boot. There appears to be no damage to the Kevlar insole. There is a 3-inch vertical tear in the leather upper on the lateral side of the heel area, and a ½-inch tear in the heel cap. There is a 2-inch lateral tear in the cushion insole. There are three small tears in the leather upper over the medial malleolus.

Shot # 26 ID # 99117-26-ALFF
M14 Mine with the improvised footwear/tire sandal
The rear one-third of the sandal has been completely destroyed and recovered in several small pieces.

Shot # 27 ID # 99117-27-BRFF
PMN Mine with improvised footwear/tire sandal
The rear one-third of the sandal has been completely destroyed with one large fragment and two smaller pieces being recovered.

Shot # 28 ID # 99117-28-BLBC
PMN Mine with blast boot/overboot combination
The outside 1-inch of the sole around the heel of the overboot has been removed by the blast, including the four heel lugs. Only a 2-½-inch x 3-inch portion of the sole is left over the mid-heel. There is a 2-½-inch longitudinal tear in the sole from heel to mid-foot. The blast deflector has been completely separated from the overboot and partially flattened down its entire length. The attenuator and attenuator plate remain attached to the
overboot, with the attenuator being completely compressed and shredded down its medial side. The Kevlar insole remains attached to the overboot and appears to be undamaged with its canvas covering being separated and shredded over the heel area. The medial and lateral halves of the Kevlar upper have been completely separated down the Achilles seam and separated from the sole from heel to mid-foot. There appears to be no damage to the Kevlar material of either half of the upper.
The sole of the blast boot has a 3-inch diagonal tear across mid-heel. This tear is split open approximately 1-inch exposing the rear portion of the blast deflector. The blast deflector, attenuator, and attenuator plate remain attached to the blast boot. There appears to have been significant flattening/compression of the blast deflector/attenuator within the sole of the blast boot. The Kevlar insole remains attached to the blast boot with the only damage being a piece of bone which has penetrated the top layers on the medial side of the heel. The leather upper has been completely separated from the sole from the rear of the heel to the arch on the medial side. The upper has been shredded by a 6-inch vertical tear extending from the sole upward on the lateral side of the heel. The cushion insole has a 2-inch longitudinal tear at mid-heel and is missing a 2-inch x 1-inch section from the medial side of the heel.
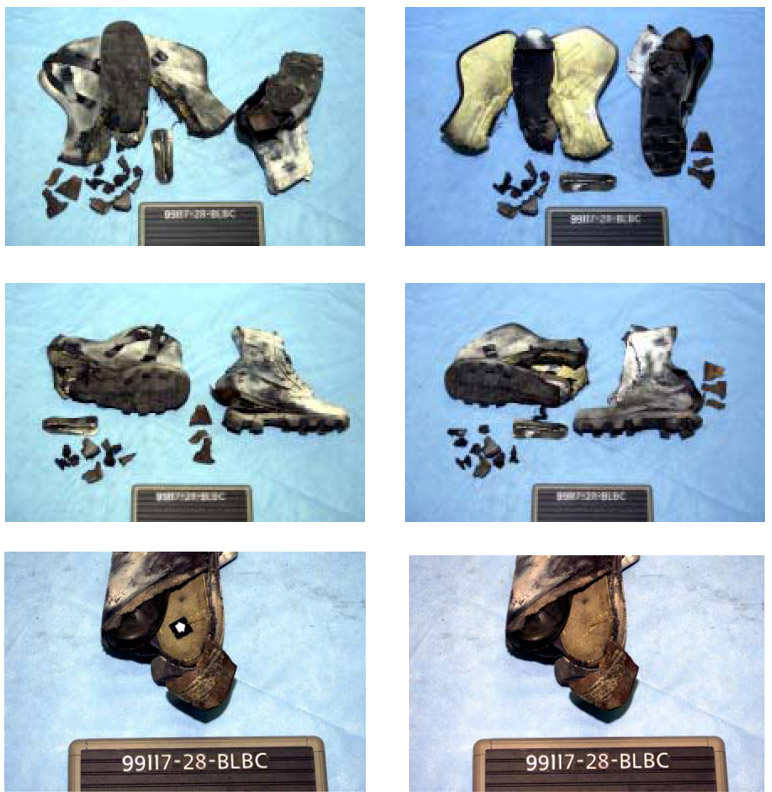
Shot # 29 ID # 99117-29-CLBD
PMA-2 Mine with blast boot/Canadian overboot combination (mine placement at mid-foot)
The Canadian overboot has sustained extensive damage with all four legs being blown off, and all four, rubber feet being separated from their respective legs. The blast deflector or underside layer of the overboot has been blown in two at mid-foot. The plate attaching the bindings to the overboot has been shattered into several small pieces resulting in the binding becoming separated from the shoe itself. The floor of the overboot has been cracked completely through at mid-foot.
There is a ½-inch tear in the leather upper of the blast boot, below the third eyelet on the lateral side. There appears to be a slight concavity of the sole of the blast boot at mid-heel, indicating possible internal compression of the deflector/attenuator.

Shot # 30 ID # 99117-30-BRBC
PMN Mine with blast boot / overboot combination.
The rear one-half of the overboot sole has been blown off. The blast deflector and attenuator have been separated from the overboot. The attenuator plate remains partially affixed to the underside of the Kevlar insole. The blast deflector has been flattened and bent upward in its center approximately one-quarter inch. The attenuator has been completely flattened and shredded and was recovered in 5 pieces. The Kevlar insole remains attached to the overboot and appears to be undamaged. The canvas covering over the Kevlar insole has been shredded in several places in the heel area. The lateral portion of the Kevlar upper has been torn from the sole to a point about two inches behind the toe, and has sustained a 4-inch vertical tear at about mid foot, with extensive shredding of the Kevlar material. The medial portion of the Kevlar upper has been separated from the sole to a point about mid-foot. Both halves of the Kevlar upper have been completely separated from each other at the Achilles seam.
The sole of the blast boot has been separated from the leather upper from heel to mid-foot, but is intact with the only apparent damage being small tears at the inside base of the heel lugs. The blast deflector has remains attached to the sole with the rear one-half being flattened. The attenuator and attenuator plate are completely separated from the boot, with the attenuator being flattened completely and the attenuator plate dented and slightly bent in the middle. The Kevlar insole has been separated from the sole from heel to mid-foot, but otherwise remains attached to the boot and is intact and undamaged. The leather upper of the blast boot has been separated from the sole from heel to mid-foot and has been badly shredded by several tears. The leather upper has a 3½-inch diagonal tear over the lateral ankle, a 4-inch tear from the sole at mid-foot to the eighth eyelet, and a 7-inch vertical tear from the sole up the Achilles seam. There are also two long vertical tears on the lateral side of the boot, one 3-inch vertical tear over the medial ankle, and one diagonal tear from the first eyelet to the arch.
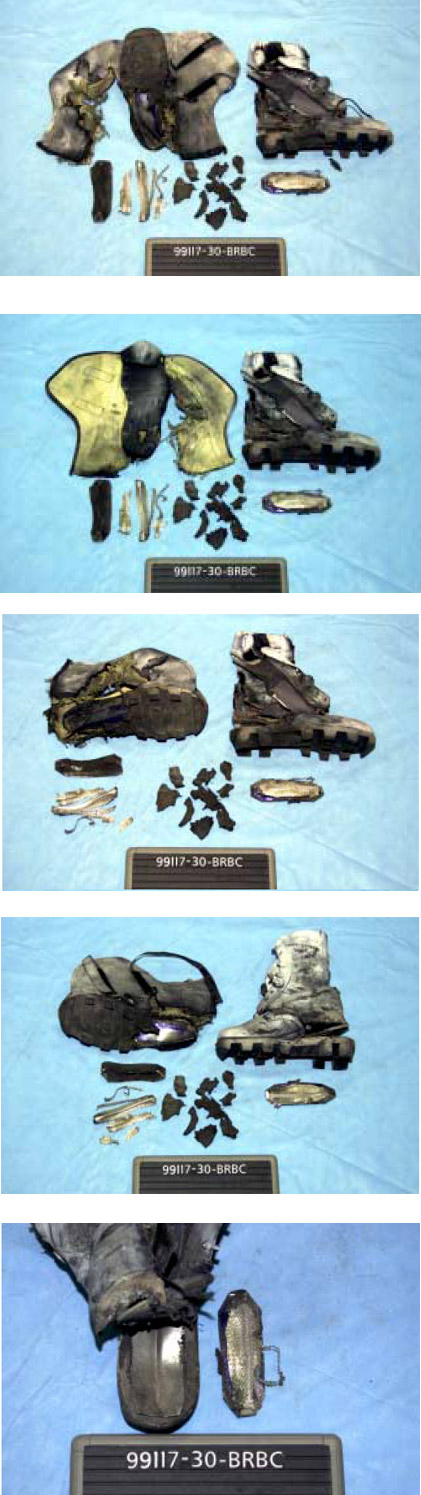
Shot # 31 ID # 99117-31-BRBD
PMN Mine with blast boot/Canadian overboot combination.
(Mine placement – left front leg)
Both of the overboot’s front legs were removed by the blast, and recovered in several small pieces. The upper portion of the legs, which remain attached the body of the boot, were badly mangled. A 3-inch x 4-inch section has been blown out of the underside of the body of the boot. The toe area of the insole has been slightly bent upward. The bindings and binding attachment plate appear to be intact and undamaged. The rubber foot of the right rear leg has been removed by the blast.
The blast boot is completely intact and appears to be undamaged.