

Article
Related Links
Eran Linder-Ganz (1), Noga Shabshin (2), Yacov Itzchak (2), Amit Gefen (1)
Dept. of Biomedical Engineering, Faculty of Engineering, Tel Aviv University Tel Aviv, Israel
*Corresponding author. Tel.: +886-4-8511888×2118; fax: +886-4-8511215.
Dept. of Diagnostic Imaging, Chaim Sheba Medical Center Tel Hashomer, Israel
Introduction
A common but serious malady afflicting wheelchair-bound and bedridden immobile patients is a deep pressure sore (DPS). Pressure sores generally develop in two separate varieties, superficial and deep. The DPS is decidedly more serious a medical complication which had motivated the present study [1]. Many researchers agree that the cause for a DPS is prolonged mechanical loads that interfere with the flow of blood and clearance of metabolic byproducts in vascularized soft tissues. A basic, first step for such investigations is to characterize the mechanical conditions in muscle and fat tissues during supported postures such as sitting. To this end, not only that data from sitting patients on the deformations, strains and stresses in deep soft tissues are missing in the literature, but there is also paucity in information on normative mechanical conditions in muscle and fat tissues during sitting. Our goal was to determine the strain and stress distributions in deep muscles and fat under the ischial tuberosities (IT) in humans during sitting in an Open-MRI. A finite element (FE) solver processed the MR images off-line, in order to obtain the two-dimensional (2D) local strain and stress tensors in muscle and fat using a “reverse engineering” approach, as detailed further.
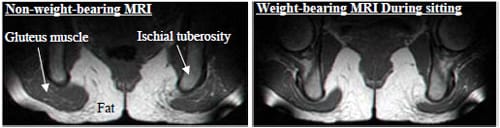
Coronal MRI images of the buttock from a healthy 29-years-old female before sitting (left) and during sitting (right)
Methods
Two male and two female healthy subjects (age: 27-29, body weight: 55-85 Kg) were recruited for this study. Imaging was performed in an open configuration MR system. The unique configuration of the open MR system allowed successful imaging during non-weight-bearing as well as weight-bearing sitting. Each subject was asked to sit comfortably, inside the MR field: first, on a rubber tire placed on the sitting surface of the system (non-weightbearing sitting) and second, directly on the sitting surface (weightbearing sitting). Interface pressures were also measured during weightbearing sitting using a pressure mat (“Tactilus”, Sensor Products Co.). For each MRI acquisition phase, the IT with their surrounding and underlying soft tissues were scanned and 2D coronal images were produced (Fig. 1). Next, a 2D FE plane stress model of the nonweight- bearing buttock geometry was developed from the non-weightbearing MRI for each subject. Each subject-specific model includes muscles, cortical bone, trabecular bone, fat and skin. Vertical sagging of the IT toward the sitting surface in a weight-bearing posture was digitally measured in each subject by comparing the two corresponding MR images. We used bone sagging measurements as displacement boundary conditions for the subject-specific FE models. Additionally, external nodes that are in contact with the sitting surface were constrained for motion in the vertical direction. After solving the FE model for these boundary conditions, we compared the contours of the deformed gluteus muscles and enveloping fat, separately for each subject, with the corresponding contours seen in the weight-bearing MR image using the least-square method (Fig. 2). By adjusting fat elastic moduli within a ±10% range, we were able to improve the fit of the FE solution to the MR image. After obtaining this best possible fit (R2>0.9, p<0.05), the FE solutions provided the local strain and stress tensors in the gluteus muscles and underlying fat for each subject.
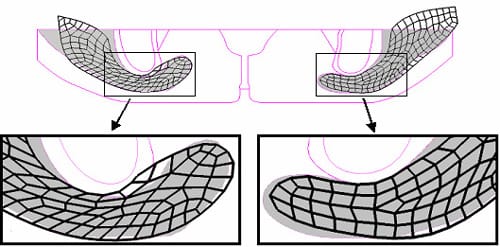
Best fit of FE-predicted gluteus muscle contours to MRI -measured muscle contours after adjusting fat stiffness to fine-tune FE model deformations
Results
Vertical sagging of the IT during sitting did not differ between the left and right sides and was 17±2mm. Peak interface pressures under the IT did not differ significantly between left and right, and were 19±3 kPa. Peak interface pressures calculated from the subjectspecific FE models overlapped with experimental data (18±4 kPa) and were statistically similar per subject, as evident from paired t-tests ran separately for the left and right body sides. Using the “reverse engineering” approach we were able to calculate the distributions of strains and stresses in muscle and fat under the IT during sitting (Table). Figure 3 demonstrates the distributions of muscle and fat strains and stresses in subject D, a healthy female (age: 29, weight: 55 Kg). Principal compressive strains and stresses in the gluteus muscle along path Mm peaked under the IT and decreased medially and laterally. Muscle strains and stresses along path Nm peaked at about 5mm from the bone-muscle interface and dropped proximally and distally from this point. Similarly, principal compressive strains and stresses in the fat layer along path Mf peaked under the IT and decreased medially and laterally. Along path Nf in fat tissue, strains and stresses were more uniformly distributed compared with muscle strain/stress on the corresponding path Nm, and decreased by about 10-15% from the most proximal to the most distal point. Generally, muscle strains and stresses were higher and less homogenous than in fat. Strain and stress distribution patterns were generally similar across subjects, i.e. peak value for both strains and stresses in gluteal muscles occurred under the IT, not directly at the bone-muscle interface but rather, 3-5mm distally. Peak strains in muscle were ~1.6-fold greater in compression and ~2.2- fold greater in tension than in fat (mean across subjects) and also, peak compressive stresses in muscle were 1.5-fold greater and less homogenously distributed than compressive stresses in fat. Interestingly, muscle tissue was subjected to considerable tension (mean of peaks across subjects ~10 kPa) but fat tissue showed negligible tension under the IT.
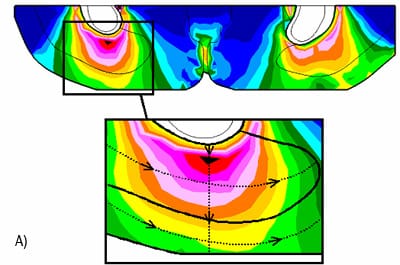
Principal compressive strains in deep tissues (fat and muscle) under the ischial tuberosities of a healthy 29-years-old female
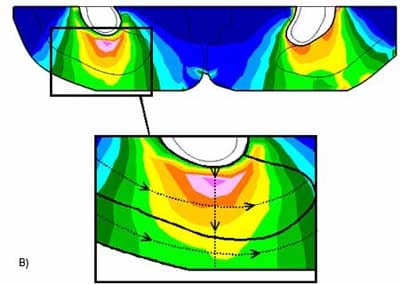
Principal compressive stresses in deep tissues (fat and muscle) under the ischial tuberosities of a healthy 29-years-old female
Discussion
We conclude that maximal tissue strains and stresses occur in the gluteal muscles, not in fat or at the skin near the body-seat interface. The results of this study have practical clinical relevancy. The pressure sores prevention industry uses the body-support interface pressure measurements to determine the stress reduction in tissues. Interface pressure mapping can be worthwhile in evaluation of the mechanical conditions on the skin but it cannot indicate on the mechanical conditions in deep soft tissues [2]. Accordingly, special supporting surfaces do not necessarily lessen internal strains and stresses in deep soft tissues [3], and the pressure relief from these products may be inefficient for DPS onset prevention. It will be extremely useful to extend the present study and test the effect of special mattress and cushions on strain and stress distributions in deep muscle and fat tissues.
REFERENCES
- Bliss, M. R., 1992, “Acute pressure area care: Sir James Paget’s legacy,” Lancet, 339, pp. 221-223.
- Gefen, A., Gefen, N., Linder-Ganz, E., and Margulies, S. S., 2005, “In vivo muscle stiffening under bone compression promotes deep pressure sores,” J Biomech Eng, 127, pp. 512-524.
- Linder-Ganz, E., and Gefen, A., 2004, “Mechanical compression-induced pressure sores in rat hindlimb: muscle stiffness, histology, and computational models,” J Appl Physiol 96, pp. 2034-2049.
