

Article
Related Links
Martin Skie, Matt Grothaus, Despina Ciocanel, Vijay Goel
Abstract
Purpose Partial wrist arthrodesis is a commonly performed procedure for the treatment of posttraumatic wrist arthritis because of its ability to provide pain relief without sacrificing complete wrist motion. The purpose of this study was to evaluate the redistribution of force after fourcorner fusion and scaphoid excision, and to correlate the findings with the reported clinical outcomes.
Methods Fifteen cadaveric wrists were used to study the biomechanics of the four-corner fusion. Pressure-sensitive film (super-low-pressure-indicating film, Sensor Products Inc, Madison, NJ) was inserted into the radiocarpal joint. Using the MTS 858 Mini Bionix (MTS System, Eden Prairie, MN), 50-kg loads (220 N) were applied to the wrists before and after simulated four-corner fusion and scaphoid excision. Statistically, we compared the pressure in the normal (intact) wrists versus four-corner fusion and scaphoid excision. The pressure measurements across the scaphoid fossa, lunate fossa, and triangular fibrocartilage complex (TFCC) were compared.
Results There is a statistical significant difference between scaphoid, lunate, and TFCC mean total force when pre and post-fusion were compared (p=0.0001). Our study revealed a statistical significant decrease in the mean scaphoid total force after scaphoid excision and four-corner fusion (p=0.0001). We also found a subsequent increase in mean total force after scaphoid excision and four-corner fusion for the lunate fossa that did not reach statistical significance (p=0.08), and no difference in load across the TFCC area (p=0.995).
Conclusions Our findings suggest that load is preferentially transferred to the radiolunate joint after scaphoid excision with four-corner fusion.
Keywords Wrist joint . Arthodesis . Biomechanics . Four-corner fusion
Introduction
Posttraumatic arthritis of the radioscaphoid and midcarpal joints is a common clinical entity resulting from joint incongruity associated with scapholunate dissociation (SLAC) or scaphoid non-union (SNAC). Because capitatehamate- lunate-triquetrum (four-corner fusion) and scaphoid excision has been shown to provide reliable pain relief while maintaining functional wrist motion, it has become a popular treatment option for arthritis resulting from scapholunate dissociation or scaphoid non-union [11].
Load mechanics of the wrist have previously been studied using pressure-sensitive film in cadaveric wrists. These studies include evaluation of the radiocarpal and midcarpal joints in a variety of positions, and under different loading conditions. Studies of the normal wrist have identified contact areas and load distribution within the proximal and midcarpal wrist joints. At the radiocarpal joint, the scaphoid transmits 60% of the load and the lunate transmits approximately 40% [9]. Across the proximal wrist joint, the radius receives 80% of the load, whereas the ulna sees 20%, as was described by Palmer and Werner. They also reported that small changes in relative ulnar length can significantly alter load patterns across the wrist. For example, with a distal radius fracture that settles 2.5 mm, an increase in ulnar axial load of approximately 40% can be expected. Palmer also demonstrated that the percentage of axial force transmitted through the ulna decreases by sequential removal of the horizontal portion of the triangular fibrocartilage complex (TFCC). This percentage decrease is accentuated with more positive ulnar variance.
The purpose of this study was to evaluate pressure distribution in the intact wrists versus four-corner fusion and scaphoid excision to determine if there is a redistribution of force to the radiolunate and ulnocarpal joints.
Materials and Methods
Contact areas and pressures within the wrist joint have been extensively studied utilizing pressure-sensitive Fuji film. Various conditions including the normal wrist in various positions under various magnitudes of load and/or load paths, various ligament injuries, fracture patterns, and various types of surgical procedures were studied. By increasing the load, the cartilage compresses, resulting in an increased contact area. The maximum load range has been found to be in the range of 200–220 N for the maximum contact area [8, 10].
Fifteen human adult wrists were harvested from cadavers. The donors included eleven females and four males with an age range of 65–94 years, with a mean of 82.2 years (standard deviation 9.03 years). The wrists were stripped of all muscles while leaving all ligaments intact. The radius and ulna were cut at 20 cm from the wrist joint and potted proximally in a polyester resin. Distally, the phalanges were removed, and the hand was potted from the metacarpal heads to the midmetacarpal level of the second through fifth metacarpals. All wrists underwent biomechanical evaluation, and all loading was performed with the wrist in a neutral position.
Before loading, a dorsal opening in the wrist capsule was made and the super-low pressure sensitive film was inserted between radius, TFCC, and the carpal bones. The two sheet-type-of-pressure-sensitive films is composed of an A film, which is coated with a particular micro-encapsulated color-forming material, and a C film, which is coated with a specific color-developing material. The film was cut to the approximate size and shape of the joint, leaving a slightly larger width than necessary dorsally to handle the film outside of the contact area. Once cut, those two sheets were placed with the coated (rough and opaque) surface opposing each other. Using a MTS System, the wrist was loaded with a 220-N force applied across the intact wrist for 5 s. The contact area resulted in red coloration on the pressure-sensitive film under the scaphoid, lunate, TFCC corresponding to contact and load the radius and ulna. After each loading test, the two sheets of pressure-sensitive film were removed from the joint, keeping only the C film.
The operative technique employed a dorsal exposure, leaving all volar radiocarpal ligaments intact. The scaphoid was excised piecemeal and a simulated limited wrist arthrodesis using K-wire stabilization of the capitate, lunate, hamate, and triquetrum was performed. The technique has been described at length in the literature [1, 12]. Pressuresensitive Fuji films were reinserted and the same load was applied. Contact areas after four-corner fusion with scaphoid excision were measured. Each wrist was loaded before and after fusion serving as its own comparison. The effects of scaphoid excision and simulated four-corner fusion on load distribution across the proximal wrist joint were studied.
After the biomechanical testing, analysis of the lowpressure- sensitive films, which generated full-color pressure maps, and accompanying statistical data, which consisted
of pressure, force, and surface area data, was performed using a 980XL Microteck scan (Topaq imagining system). The system consists of a specially calibrated scanner and the Topaq Pressure analysis System (Sensor Products, Inc., Madison, NJ). Used in conjunction with pressure-indicating Fuji films, Topaq pressure analysis system provides a quick analysis of the pressure distribution and surface area of any two surfaces that come into contact, generating full-color pressure maps and accompanying statistical data, which consisted of pressure, force, and surface area data.
The Topaq imaging system also allowed cropping of the scanned areas, enabling direct focus on specific regions of interest. We divided each film in three areas of interest corresponding to the: scaphoid fossa, lunate fossa, and TFCC. The areas of division were determined by two separate investigators. Pressure-sensitive Fuji film is directly related to the amount of pressure applied to it. Figure 1 shows a pressure-sensitive Fuji film with increasing red coloration corresponding to increased load in intact wrist and after four-corner fusion. The Topaq system read and interpreted pressure, assimilating it in an easy to read format. The system uses a color correlation to analyze the data (Fig. 1).
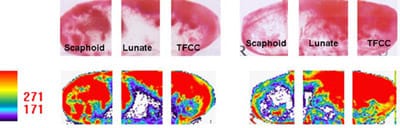
Figure 1. Fuji pressure sensitive films and color conversion in intact wrist and after four-corner fusion.
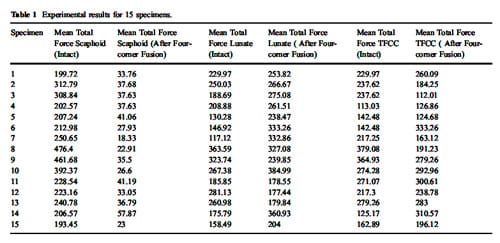
Data were collected for each area (scaphoid, lunate, TFCC), and repeated ANOVA analyses compared the pressure loads in three regions: scaphoid, lunate, TFCC on intact wrists versus scaphoid excision with simulated four-corner fusion (Table 1). A p value of less than 0.05 was considered to be statistically significant.
Results
The pressure-sensitive Fuji film data can be utilized to show the changing pattern of contact on the radius comparing a pressure sensitive film of a normal wrist in neutral position with the pattern of contact after scaphoid excision with four-corner fusion. The pressure-sensitive Fuji film has increasing red coloration with increasing load. Results form the Topaq software analysis revealed the mean total force for the intact scaphoid fossa was 274.51 N, (SD 96 N), mean total force for the intact lunate fossa was 219.25 N (SD 71.72 N), and for the intact TFCC a mean total force was 226.29 N (SD 80.72 N).
The mean total force for scaphoid fossa after scaphoid excision and simulated four-corner fusion was 34.06 N (SD 9.6 N), for lunate fossa 267.62 N (SD 67.77 N), and 226.45 N for TFCC (SD 74.16 N). The mean difference is statistically significant at the 0.05 levels for change in pressure across the scaphoid fossa.
The following graph shows the mean force in Newtons (N) for the intact wrist compared to scaphoid excision and four-corner fusion (Fig. 2).
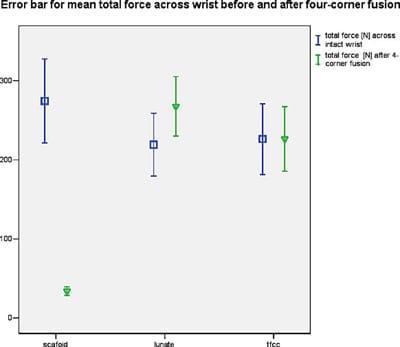
Figure 2. Error bars for the mean force (N) in intact wrist versus scaphoid excision with four-corner fusion.
Repeated ANOVA was performed to compare the mean total force across three areas: scaphoid fossa, lunate fossa, and the TFCC in intact wrists and postfusion wrists. We found a statistically significant decrease in mean total force for the scaphoid fossa after scaphoid excision and fourcorner fusion (p=0.0001). There is a statistically nonsignificant increase in the load on the lunate fossa (p=0.08), and no appreciable change in the mean total force within the TFCC area (p=0.99).
Discussion
Studies of pressure-sensitive studies have revealed that the areas of increased load coincide with areas that develop joint space narrowing and arthritis in the clinical setting, and result in the scapholunate advance collapse (SLAC) wrist. Pressure film studies have also revealed a strong correlation between increased load at the distal scaphoid fragment and the radial styloid, coinciding with the area where degenerative changes are seen in a long-standing scaphoid non-union (SNAC). These studies also show a decrease, or no change, in load under the proximal pole of the scaphoid and the lunate in wrists with scaphoid non-union, again correlating to clinical findings where the proximal scaphoid fossa and lunate fossa of the radius are maintained and do not tend to develop degenerative changes, even in a long-standing non-union of the scaphoid [8].
With this biomechanical study of intact wrist versus four-corner fusion with scaphoid excision, we demonstrated that there is a statistically significant decrease in the load across the scaphoid fossa. Clearly, in the clinical setting, excision of the scaphoid would be expected to provide relief of pain resulting from bone-to-bone contact in the arthritic scaphoid fossa, and dramatically decrease the load transmitted across the fossa. Our finding supports those by Kobza et al. [5], which revealed that after four-corner fusion with scaphoid excision, there is a significant decrease in contact pressure in the scaphoid fossa, and a concomitant increase in mean radiolunate contact pressure compared with the intact specimen (p<0.01). We also found a mean increase in total force within the lunate fossa, although not reaching statistical significance (p=0.08), and a nonsignificant increase for the TFCC area (p=0.89).
Clinical studies done by Cohen et al. [3] concluded that pain relief was equivalent for proximal row carpectomy and fourcorner fusion, both methods being motion-preserving options for the treatment of SLAC arthritis. Multiple clinical studies reported successful pain relief with comparable results in terms of both motion and strength [2, 6, 7, 11, 13]. Fourcorner arthrodesis provides a satisfactory option for palmar midcarpal instability [4]. No clinical study had made note of a significant increase in ulnar-sided wrist pain, as one may expect because of redistribution of load from that normally would be transferred across the radioscaphoid joint.
Our findings also suggest that load across the radioscaphoid joint is preferentially redistributed to the radiolunate joint as compared to the ulnocarpal articulation. This finding may help to explain why the clinical results after scaphoid excision and four-corner fusion and proximal row carpectomy are so comparable, as were reported by Cohen [3] and Wyrick [13].
Our study supports the findings of Kobza et al. [5]. Kobza reported a significant increase in mean radiolunate contact pressure when compared with the intact specimen, whereas our study revealed an increase for the mean total force for the lunate fossa, although not achieving statistical significance. However, Kobza et al [5] did not evaluate the extent to which load was transferred to the TFCC and ulnocarpal joint. Our findings show nonsignificant increase in load on the TFCC after scaphoid excision and fourcorner fusion. We feel that these findings are clinically important, and may help explain the long-term pain relief achieved after this surgical procedure.
As with prior studies, our findings also demonstrate some of the limitations of the use of pressure-sensitive film. Figure 2 Error bars for the mean force (N) in intact wrist versus scaphoid excision with four-corner fusion. HAND (2007) 2:194–198 197 After complete excision of the scaphoid, the force across the scaphoid fossa did not decrease to zero. There was artifact created by pressure from the dorsal and volar rims of the scaphoid fossa during loading. Another source of potential error occurs in dividing the image i
nto the sections to be studied, although every effort was taken to assure that the divisions were consistent between compared images.
The purpose of this study was to evaluate pressure distribution in the intact wrists versus four-corner fusion and scaphoid excision, and to correlate the findings with the clinically reported pain relief after this procedure. It has been our experience that there is not a significant increase in ulnar sided wrist pain after four-corner fusion, nor was ulnar sided pain noted in the above mentioned reports.
REFERENCES
- Ashmead D, Watson HK. SLAC wrist reconstruction. Master techniques in orthopaedic surgery. In: Gelberman RH, editor. The wrist. New York: Raven Press; 1994. p. 319–30.
- Ashmead D, Watson HK, Damon C, Herber S, Paly W. Scapholunate advanced collapse wrist salvage. J Hand Surg 1994;19A:741–50.
- Cohen MS, Kozin SH. Degenerative arthritis of the wrist: proximal row carpectomy versus scaphoid excision and fourcorner arthrodesis. J Hand Surg 2001;26(1):94–104.
- Goldfarb CA, Stern PJ, Kiefhaber TR. Palmar midcarpal instability: the results of treatment with four-corner arthrodesis. J Hand Surg 2004;29(2):258–63.
- Kobza PE, Budoff JE, Yeh ML. Management of the scaphoid during four-corner fusion—a cadaveric study. J Hand Surg 2003;28(6):904–9.
- Krakauer JD, Bishop AT, Cooney WP. Surgical treatment of scapholunate advanced collapse. J Hand Surg 1994;19(5):751–9.
- Tomaino MM, Miller RJ, Cole I, Burton RI. Scapholunate advanced collapse wrist: proximal row carpectomy or limited wrist arthrodesis with scaphoid excision? J Hand Surg 1994;19A:134–42.
- Viegas SF, Patterson RM. Load mechanics of the wrist. Hand Clinics 1997;13(1):109–28.
- Viegas SF, Patterson R, Peterson P, Roefs J, Tencer A, Choi S. The effects of various load paths and different loads on the load transfer characteristics of the wrist. J Hand Surg 1989 May;14 (3):458–65.
- Viegas SF, Patterson RM, Werner FW. Joint contact area and pressure. In: An K-N, Berger RA, Cooney WP III, editors. Biomechanics of the wrist joint. Springer, Berlin Heidelberg New York; 1991. p. 99–126.
- Watson HK, Ballet FL. The SLAC wrist: scapholunate advanced collapse pattern of degenerative arthritis. J Hand Surg 1984;9 (3):358–65.
- Watson HK, Goodman ML, Johnson TR. Limited writ arthrodesis. Part II: Intercarpal and radiocarpal combinations. J Hand Surg 1981;6:223–33.
- Wyrick JD, Stern PJ, Kiefhaber TR. Motion-preserving procedures in the treatment of scapholunate advanced collapse wrist: proximal row carpectomy versus four-corner arthrodesis. J Hand Surg 1995; 20A:965–70.
