

Article
Related Links
Richard F. Edlich, MD, PhD, FACEP, FACS, FASPS,1 Shelley S. Mason, BS,2 Rober J. Vissers, MD, FACEP,3 K. Dean Gubler, DO, MPH,4 John G. Thacker, PhD, 5 Paul Pharr, RN, CFN, 6 Mark Anderson, Rn, TNC,7 William B. Long III, MD, FACS, FASTS,8
1Distinguished Professor Emeritus of Plastic Surgery, Biomedical Engineering and Emergency Medicine, University of Virginia Health System, Director of Trauma Prevention, Education and Research at Legacy Verified Level I Shock Trauma Center for Pediatrics and Adults, Legacy Emanuel Hospital, Portland, OR (USA) 2Information Specialist, Legacy Emanuel Hospital, Portland, OR (USA) 3Medical Director, Emergency Department, Legacy Emanuel Hospital, Portland, Or. (USA) 4Surgical Critical Care Director, Legacy Verified Level I Shock Trauma Center for Pediatrics and Adults, Legacy Emanuel Hospital, Portland, OR (USA) 5Assistant Chairman, Department of Mechanical and Aerospace Engineering, University of Virginia, Charlottesville VA (USA) 6Trauma Nurse Coordinator, Legacy Verified Level I Trauma Center, Legacy Emanuel Hospital, Portland OR. (USA) 7Director of Education and Clinical Outreach for Life Flight Network, Portland, OR. (USA) 8President and Medical Director of Medical Specialists, LLP., Legacy Verified Level I Shock Trauma Center for Pediatrics and Adults, Legacy Emanuel Hospital, Portland, OR (USA)
ABSTRACT
Patients with suspected spinal cord injury are immobilized to a backboard during ambulance and helicopter air transport. It has been well documented that patients that are immobilized to a backboard are susceptible to pressure ulcer formation. Due to the significant amount of time an average patient with a suspected spinal cord injury spends on a backboard, it is imperative to prevent pressure ulcer formation. Realizing the dangers of the potentially preventable pressure ulcers, our team of scientists, surgeons, and trauma nurses, performed a comprehensive study of the Back Raft system that was designed to reduce patient discomfort and skin interface pressure. Using ten healthy volunteers, we documented that the Back Raft significantly reduces discomfort as well as tissue interface pressure in the occipital, scapula, and sacral regions of the back. Recognizing the benefits of using the Back Raft system in prevention of pressure ulcer formation, we now routinely use this device for patients being transported to our trauma center and emergency department. The implementation of an inflatable mattress conjointly with a backboard is particularly important to the financial stability of hospitals that care for patients that are susceptible to developing preventable hospital acquired conditions. In 2008, The Centers for Medicare & Medicaid Services (CMS) enacted a policy in which the CMS can refuse payment for hospital acquired conditions. Pressure ulcers were among the hospital acquired conditions within the final rule. Prevention of pressure ulcers can save hospitals millions of dollars each year.
Keywords—Back Raft inflatable air mattress, backboard, pressure mapping, surface contact area (SCA), interface pressure, pressure ulcer
INTRODUCTION
In 1979, a team of nurses, trauma surgeons, and neurosurgeons wrote one of the first comprehensive reviews on the prehospital treatment of patients with spinal cord injuries (1). In this clinical report, the authors pointed out that the lowered morbidity and mortality rates of patients suffering spinal cord injuries (SCIs) can be traced to improved techniques in patient care in the prehospital phase of the system. One of the highlights of the prehospital care of a patient with a spinal cord injury was to stabilize the patient before transport. It was pointed out that the cardinal principal in moving a patient with a suspected spinal cord injury (SCI) was to prevent any motion of the spinal column that can further damage the spinal cord or nerve roots. This stabilization can be accomplished by immobilizing the patient’s head, neck, and back, to a backboard prior to transport.
Although SCI is uncommon in the relation of total preshospital patient encounters, up to 20,000 cases may occur annually in the United States and Northern Europe (2). It is estimated that between 500-700 people in the United Kingdom and 10,000 people in the United States sustain a traumatic spinal cord injury each year (3). Acute traumatic SCI occurs in about 3% of trauma admissions to hospitals, and half these injuries involve the cervical spine (3). SCI can result in long-term disability, often with profound effects on the quality of life.
Backboards are routinely used throughout the world as a means of spinal immobilization during the course of trauma patient care. Immobilizing patients with backboards is a common procedure utilized by Emergency Medical Technicians and Paramedics for all patients with SCIs (4). These patients are fully immobilized prior to transport to the emergency department or trauma center, regardless of presenting signs or symptoms. Many studies have shown that this is a potential source of patient discomfort and pressure ulcer formation (4, 5). Several studies have also shown that immobilizing noninjured, healthy patients for 30 to 80 minutes on a backboard causes most subjects to have pain and discomfort (4). Lerner and Moscati point out in a prospective study that a patient spends an average 77 minutes on a backboard (4).
Pressure ulcer development in patients with SCI is a problem of great clinical significance. Sheerin and Frein estimated that pressure ulcers will develop in up to 40% of patients in the immediate post injury period and up to 80% of patients overall (5). The National Pressure Ulcer Advisor Panel defines a pressure ulcer as the disruption of normal and anatomic structure and function of the skin that results from external force associated with a bony prominence and does not heal in an orderly and timely fashion (6). Realizing the potential dangers of pressure ulcer development in patients immobilized to a backboard, a team of trauma surgeons, emergency medical technicians, and scientists provided scientific information on the performance of a revolutionary, inexpensive spinal board immobilization system, the Back Raft, developed by MediTech, Inc., distributed by Thomas EMS (Salt Lake City, Utah), that can dramatically reduce patient discomfort and skin interface pressure during transport of a patient stabilized to a backboard. This report has the following components: 1. A detailed description of the Back Raft system, highlighting how it is attached to the backboard; 2. A narrative description of the technology of measuring patient discomfort on a standard backboard compared to that of a standard backboard with a Back Raft mattress; 3. A review of the s
kin interface measuring system for patients lying on a backboard as well as the same patients lying on a backboard containing a Back Raft; 4. The results of the level of discomfort and pressure mapping measurements of the occipital, scapula, and sacral regions of the back; and finally 5. A discussion of the potential impact of pressure ulcer development on patients immobilized to a backboard, including malpractice liability, as well as reimbursement implications to the Emergency Department or Trauma Center.
The Back Raft System
The Back Raft is an inflatable air mattress and spinal stabilization apparatus that is applicable to a standard spinal backboard (compatible with 16” and 18” backboards). It provides additional support in order to improve patient comfort and reduce the risk of pressure ulcers and other secondary injuries during transport. The fundamental design of a standard spinal backboard is to immobilize an injured patient’s spinal column from mechanical and rotational movement in order to prevent additional trauma to the potentially injured spine, ligaments, and neuronal structures that comprise the spinal cord (3). The Back Raft mattress provides additional static mechanical support during patient transport.
Because the hard surface of a backboard produces high interface pressures between the skin and the spinal backboard, the Back Raft was designed to reduce the pressure to critical pressure points by the inflation of seven columns that support the shoulders and lower back. In addition, there are three columns of air support that stabilize the head and neck, reducing the pressure point on the back of the head, while increasing the effectiveness of spinal immobilization.
The Back Raft is applied and remains on the backboard prior to a patient being immobilized on a backboard. Before inflation the Back Raft conforms to the backboard for easy storage on an ambulance or helicopter air medical transport. The Back Raft can be inflated with a hand pump within seconds, filling the space between the patient and the backboard, relieving the stress on tissue interface pressures. The function of the backboard is not compromised when the mattress is fully inflated, allowing transport of a patient to maintain the same level of efficiency.
The purpose of our study was to record the level of patient discomfort and to measure the tissue-interface pressures at the occipital, scapula, and sacral, surface contact area of the standard backboard as well as on the backboard with a Back Raft system attached.
Materials and Methods
Ten healthy volunteers who had not taken any pain medications in the preceding 24 hours, and were not experiencing any back pain of any kind, were studied on a backboard in two separate trials, lying on a backboard without a Back Raft, and then on a backboard with a Back Raft attached. Of the ten healthy volunteers five (50%) were men and five (50%) women, with an average age of 45.3 (range 33-59). Height and weight of the volunteers were measured to calculate the body mass index (BMI) and pound-to-inch ratio (Table 1) (7).
Volunteers were placed horizontal on a wooden back board that was placed on a three foot high wooden assembly. The backboard used was a 16” wide XTRA backboard manufactured by Allied Healthcare Products Inc. (St. Louis, MO). The volunteers were studied for 30 minutes on a backboard without the Back Raft, and then allowed off the board for 30 minutes to rest. They were then studied for a second 30 minute interval on a backboard with a Back Raft support attached.
Level of pain was measured at baseline (time 0) and at 15 minute intervals (15 and 30 minutes). At the end of each 15 minute period, subjects were asked to assess the tested surface for comfort on a 10-point visual analog scale (VAS). The horizontal visual analog scale was measured from 1 to 10 with one being “no pain” and ten being “worst possible pain.” After each interval, the subject was asked to rate comfort. Interface or contact pressures between the subject and board or Back Raft were measured at the occipital, scapula, and sacrum with a Tactilus® pressure evaluator. An average of pressure in mmHg was obtained at each location (Occipital, scapula, and sacrum) at baseline and at 15- minute intervals. After the subject’s height and weight was recorded, we determined BMI by dividing weight by height (pounds-per-inch ratio).
Surface contact areas (SCA) of a standard spinal backboard (16” wide XTRA backboard manufactured by Allied Healthcare Products) and the Back Raft were compared in 10 volunteers. Each subject’s examination resulted in a computer-generated diagram indicating the pressure distribution in each SCA (occipital, scapula, and sacral regions) on a Back Raft and on the standard backboard without a Back Raft. The evaluation was performed by using a computerized system that collects pressure data. The tactile pressure mapping sensor system shows how the pressure and body temperature are distributed, and the magnitude of pressure occurring.
Statistical analysis was performed comparing t test for the two groups using Microsoft excel (2007). According to this analysis, a number of ten volunteers in each group would provide a study with a power of 95%. For all statistical tests, a p value ≤0.05 was considered significant.
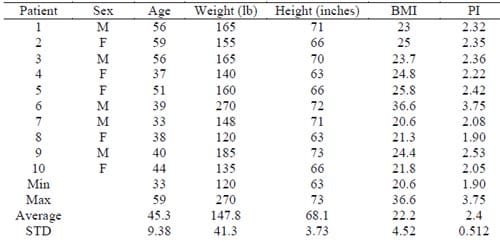
Table 1: Volunteers General Data
Results
Of the 10 volunteer studied, 5 (50%) were female and 5 (50%) were male. The average age was 45.3 years (SEM, 2.97; range 33 to 59), the average height was 68.1 inches (SEM, 1.18; range 63 to 73), the average weight was 147.8 pounds (SEM, 13.06; range 120 to 270), and the average pound-to-inch ratio was 2.4 (SEM, 0.16; range 1.90 to 3.75).
Pain measurements and interface pressure levels are reported in Table 2. The mean pain was 6.0 at the end of the period with no Back Raft and 0.9 at the end of the period with the Back Raft (P=<0.05). These measurements indicate that pain levels changed significantly over time (P=<0.05) and that the backboard by itself differed significantly in amount of pain than with the Back Raft attached (P=<0.05). All subjects reported that the Back Raft was “much more comfortable” than being immobilized on the backboard itself.
Interface pressure levels were significantly higher during the period with the backboard without the Back Raft mattress attached then during the period with the Back Raft at the occipital (P=<0.05), scapula (P=<0.05), and sacral (P=<0.05).
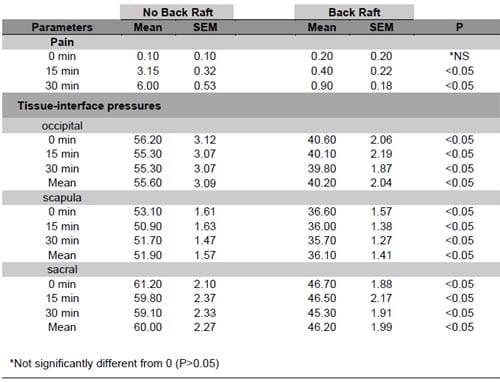
Table 2. Pain measurement and interface pressure levels
Discussion
Our findings demonstrated that the Back Raft provided relief of the tissue interface pressures of the occipital, scapula and sacral regions of the back. In addition, the Back Raft system significantly reduced patient discomfort while lying on a backboard.
In United States, backboards are routinely used to immobilize patients with suspected spinal cord injuries. Backboards are a critical component of the advanced traumatic life support protocol (8). The practice of prehospital spine immobilization has been adopted as a standard Emergency Medical Service (EMS) practice for trauma patients in the United States and many other countries (9). Burton et. al reported that injury attributed to the immobilization intervention, including pain and discomfort, pressure sore development, respiratory compromise, and inadequate spine immobilization, is cited as a substantial consequence that outweighs the potential benefit derived form routine EMS immobilization of trauma patients (9
).
In Kwan and Bunns systematic review of prehospital spinal immobilization they found that there was a significant improvement in comfort associated with the use of vacuum mattress splints compared with wooden backboards. The medical and legal concern of missing a spinal cord injury has lent strong support for the conservative approach of liberal prehospital spinal immobilization to almost all patients with trauma and possible neck injury, regardless of clinical complaint (3). The adverse effects of immobilization on a backboard of patients with suspected spinal cord injury, especially pressure ulcer formation, have been well documented.
A pressure ulcer is defined as an area of tissue damage appearing after a prolonged period of ischemia in the tissue. There are several factors that contribute to the formation of pressure sores. Extrinsic factors are externally applied pressure, shear forces and increases in surface temperature and humidity (10). Most researchers agree that the primary cause of pressure sores is externally applied pressure, leading to ischemia (10). Pressure ulcers develop at bony sites where sustained pressure results in compromised perfusion, ischemia and necrosis (11). Low grade ulcers can appear in as few as two hours (11). As many as 3 million adults have at least one pressure ulcer, with an estimated cost of treatment being from $500-$70,000 per ulcer (12). The United States spends an estimated $11 billion dollars per year on pressure ulcers, 60% of which begin during acute care admissions (13).
In 2007, a special advisory came out that the Center for Medicare and Medicaid Services (CMS) released a final rule for its fiscal year 2008 hospital inpatient prospective payment system. CMS announced its decision to cease paying hospitals for some of the care made necessary by “preventable complications”—conditions that result from medical errors or improper care and that can reasonably be expected to be averted (14). This rule implements a congressionally mandated change in hospital reimbursement. Pressure ulcers were listed under hospital acquired conditions that would fall within this new rule.
In 2006 it was reported that there was 322,946 Medicare cases of pressure ulcers with an average payment for admissions being $40,381 (14). As of October 1, 2008 medical conditions, if not present at the time of admission, are no longer calculated in the payments to the hospitals (14).This rule has resulted in hospitals seeing substantial reductions in payment for the care of individual patients with preventable complications.
Because of CMS’s new policy there has been new strategies implemented to prevent hospital acquired conditions. Daily skin assessments, maximized nutrition and repositioning are some of the key strategies in published guidelines and hospital protocols for pressure ulcer prevention (15-16). It was reported that the incidence of pressure ulcers acquired in the hospital have decreased from 6.1% to 3.9% between May 2007 and March 2008 (16). With this new policy in place, physician and staff involvement in hospital acquired conditions is imperative. Utilizing a mattress system such as the Back Raft during medical emergencies and trauma accidents in which a backboard is employed is taking prevention to a prehospital level that is necessary for avoiding hospital acquired conditions such as pressure ulceration.
Realizing the benefits of the Back Raft system, the Life Flight air transport system in the Pacific Northwest uses this system to transport the immobilized patients in their helicopter air transport system. At the present time, Life Flight uses the Back Raft system on patients whose air transport time will exceed one hour. If the Back Raft system were being used in all hospitals and ambulance services, then the patient with a suspected spinal cord injury would be immobilized on a backboard with Back Raft to facilitate transport by either ambulance or air transport at sites that are less then 60 minutes from a Trauma Center or Emergency Department. Appreciating the importance of the Back Raft system in transporting patients that are immobilized to a backboard, we are now expanding emergency medical training to paramedics and emergency medical technicians who transport patients in ambulances.
DISCLAIMER – All of the authors of this report have not received any financial remuneration or financial support for this study.

Figure 1: The inflated Back Raft System attached to a standard backboard and inflation hand pump.

Figure 2: Volunteer immobilized on inflated Back Raft system attached to a standard backboard.
REFERENCES
- Rimel, R., Winn, R., Rice, P., Butler, A., Edlich, R., Buck, R., Jane, J. Prehospital treatment of the patient with spinal cord injuries. EMT J. December 1979;51-54.
- Hostler D, Colburn D, Seitz SR. A comparison of three cervical immobilization devices. Prehosp Emerg Care. 2009;13(2):256-60.
- Kwan I, Bunn F. Effects of prehospital spinal immobilization: a systematic review of randomized trials on healthy subjects. Prehosp Disaster Med. 2005;20(1):47- 53. Review.
- Lerner B, Moscati R. Duration of patient immobilization in the ED. Duration of patient immobilization in the ED. Am J Emerg Med. 2000;18(1):28-30.
- Sheerin F, de Frein R. The occipital and sacral pressures experienced by healthy volunteers under spinal immobilization: a trial of three surfaces. J Emerg Nurs. 2007;33(5):447-50.
- Marglois DJ. Definiation of a pressure ulcer. Adv Wound Care.1995:8:8-10.
- Wilder RP, Greene JA, Winters KL, Long WB 3rd, Gubler K, Edlich RF.Physical fitness assessment: an update. J Long Term Eff Med Implants. 2006;16(2):193- 204.
- Kosashvili Y, Backstein D, Ziv YB, Safir O, Blumenfeld A, Mirovsky Y. A biomechanical comparison between the thoracolumbosacral surface contact area (SCA) of a standard backboard with other rigid immobilization surfaces. J Trauma. 2009;66(1):191-4.
- Burton JH, Dunn MG, Harmon NR, Hermanson TA, Bradshaw JR. A statewide, prehospital emergency medical service selective patient spine immobilization protocol. J Trauma. 2006;61(1):161-7.
- Jonsson A, Lindén M, Lindgren M, Malmqvist LA, Bäcklund Y. Evaluation of antidecubitus mattresses. Med Biol Eng Comput. 2005 Sep;43(5):541-7. Review.
- Dini V, Bertone M, Romanelli M. Prevention and management of pressure ulcers. Dermatologic Therapy 2006;19(6), 356-364.
- Reddy M, Gill S, Rochon P. Preventing pressure ulcers: A systematic review. JAMA. 2006;296(8):974-984.
- Kuhn B. Balancing the pressure ulcer cost and quality equation. Nurs Econ. 1992; 10:353-359.
- Rosenthal M. Nonpayment for performance? Medicare’s new reimbursement rule. N Engl J Med. 2007;357(16):1573-1575.
- Bergstrom N, Allman R, Carlson C. Clinical practice guidline number 3: Pressure ulcers in adultsL prediction and prevention. Rockville, Md: Public Health Service, US Dept of Health and Human Services; 1992.
- Cuddigan J, Ayello E, Sussman C, Baranoski S. Pressure ulcers in America: Prevalence, incidence, and implications for the future. Reston, Va: National Pressure Ulcer Advisory Panel; 2001.
