

Article
Related Links
Thay Q. Lee, PhD; Matthew D. Sandusky, BS; Arshya Adeli, BS; Patrick J. McMahon, MD
Orthopaedic Biomechanics Laboratory, Veterans Affairs Healthcare System, Long Beach, CA; Department of Orthopaedic Surgery, University of California, Irvine, CA
Abstract
Selective strengthening of the vastus medialis (VM) muscle is a conservative treatment used to address some patellofemoral joint (PFJ) problems. The objective of this study was to examine the effects of varying VM strength on PFJ kinematics and contact pressures and areas. We tested five fresh-frozen cadaveric knees using a custom knee jig, which permits the simulation of physiologic quadriceps loading while also allowing the VM force to be varied. PFJ kinematics were measured with a magnetic tracking device. PFJ contact pressures and areas were measured with Fuji pressure-sensitive film. For PFJ kinematics, the change in the medial-lateral and superior-inferior translation was significant at 0% of VM strength and 150% of VM strength with respect to the 100% of VM strength condition (p < 0.05). Extreme changes in the VM force had a statistically significant effect on patellofemoral contact pressures (0% of VM strength (19 ± 10%) and 150% of VM strength (17 ± 3%) with respect to 100% of VM strength condition (p < 0.05)). No statistically significant differences were shown in the patellofemoral contact areas (p > 0.05). The functional range of VM strength is between 75% and 125% of total VM strength. The PFJ kinematics and contact pressures were not significantly influenced by VM strength except at extreme conditions (0% of VM strength or 150% of VM strength) in human cadaveric knees.
Keywords: biomechanics, cadaver, contact pressures, patellofemoral joint, vastus medialis strength.
Introduction
The patella is an essential component of the knee. Its most important function is to extend the knee by increasing the distance of the extensor apparatus from the axis of flexion and extension of the knee. Other functions of the patella include controlling the capsular tension in the knee and protecting the cartilage of the trochlea as well as the condyles.
Proper alignment and restoration of the kinematic variables in the patellofemoral mechanism are essential for adequate functioning and longevity of this joint. As the knee flexes, the retropatellar contact moves from the inferior surface to the superior surface [1]. This movement of the retropatellar contact produces noncentral loading of the patella in a wide range of functional activities. The maximum loads on the retropatellar surface essentially cover the entire articular surface during normal daily activities [1]. However, abnormal patellofemoral kinematics will cause eccentricity of the retropatellar surface to increase, resulting in patellofemoral joint (PFJ) pathology [1–4].
The pathophysiology of patellofemoral pain is poorly understood [5,6]. One etiology for anterior knee pain is quadriceps atrophy and/or weakness, particularly the vastus medialis (VM), which leads to an imbalance and maltracking of the patella, resulting in knee pain and/or instability [7–10]. The line of pull of the quadriceps is relatively valgus with respect to the joint line of the knee [11,12]. This tends to favor lateral deviation, even if the anatomy is completely normal [10]. The VM has an important role as a medial stabilizer of the patella and aids in the normal functioning of the PFJ [8,13,14]. The VM is phylogenetically the weakest of the quadriceps group and appears to be the first muscle to atrophy and the last to rehabilitate [10,15,16]. Quadriceps strengthening exercises, emphasizing the VM, have been suggested as the primary initial management of patellofemoral disorders [6,17–23]. This treatment, however, has yielded inconsistent results clinically.
Researchers have studied the mechanism of the PFJ extensively in the past by determining quadriceps force with respect to various physiological activities [24–26]. The earlier approaches to determine various forces on the PFJ assumed that the patella mechanism was a frictionless pulley system, and the forces were then calculated from indirect measurements [26,27]. This assumption was unrealistic for the patella force system, since the ratio between PFJ reaction force and the quadriceps tension vary in a complex manner with respect to the knee flexion angle [1,25,28,29]. Ahmed et al. in 1987 performed an extensive analysis of the PFJ reaction force and the tension in the ligamentum patellae as a function of the predetermined quadriceps force and the geometry of the patellar system [1]. Earlier, in 1984, Huberti and Hayes studied patellofemoral contact pressures in human cadaveric knees by using Fuji pressuresensitive film for intra-articular contact pressures [2]. These authors found that in normal human joints, despite their complex surface geometry and loading mechanism, the patellofemoral contact pressures were remarkably uniform over a wide range of motion. In addition, deviations from the normal quadriceps angle (Q angle) were associated with increased peak patellofemoral pressures and unpredictable patterns of cartilage unloading. In 1988, Huberti and Hayes again used Fuji pressure-sensitive film to show the relationship of the maximum patellofemoral contact pressures with respect to knee flexion angle and tibial rotation [3]. Garg and Walker in 1990 reported on the geometry and knee motion using human cadaver knees and developed an algorithm for patellar motion [30]. Heegaard et al. reported on the contribution of geometry and soft tissue structures on patellar stability [31]. These authors reported that the guiding role of the femoral groove prevailed over soft tissue structures in patellar stability.
In cadaver studies, Ahmed et al. in 1983 showed that the removal of the vastus medialis obliquus (VMO) tension shifted the pressure zone from the center to the lateral facet of the patella [28]. Similarly, Goh et al. in 1995 reported that the absence of VMO caused the patella to displace laterally and increased the load on the lateral patellar facet throughout the range of knee motion [32]. However, these authors used wires to simulate the five muscle bellies of the quadriceps and determined the ratio of their tensions from the anatomical cross-sectional area of the muscles.
The objective of this study was to examine the effects of VM strength variation on the patellofemoral contact areas and pressures as well as the patellar translations at knee flexion angles of 0°, 30°, 60°, and 90° in human cadaver knees. For this to be accomplished, anatomically based muscle loading direction described by Powers et al. [33] and the simulated muscle force ratio based on physiological muscle cross-sectional area reported by Wickiewicz et al. [34]
were used with a custom PFJ testing jig.
Materials and Methods
Specimen Dissection and Clamping
Five fresh-frozen, unmatched cadaveric knees were used in this study. We examined all knees before testing both macroscopically and radiographically to eliminate specimens with any prior trauma, surgery, and/or arthrosis. The cadaver specimens ranged from 60 to 80 years of age. The tibia and femur were cut to approximately 20 cm long for mounting. We removed skin and subcutaneous fat while carefully preserving the joint capsule and the surrounding retinaculum. All musculature was dissected and removed from the tibia as well as the posterior femur. We then cut the fibula near the level of its articulation with the tibia preserving the insertion of the lateral collateral ligament by fixing the fibula to the tibia with a 3.5- × 24-mm cortical screw.
We separated the individual components of the extensor mechanism, the VM, vastus lateralis (VL), vastus intermedius (VI), and rectus femoris (RF) from each other using the fascial planes between the muscles as a guide. The iliotibial band (ITB) was also isolated. The vasti were then reflected from their posterior origin (linea aspera). Once we reflected the quadriceps anteriorly from the femur, we opened the suprapatellar pouch to access the PFJ for the intra-articular measurement of contact pressures and areas. For all structures, insertions into the patella, patellar tendon, and peripatellar retinaculum were carefully preserved. We then trimmed the individual muscles to accommodate the width of the clamps used for applying the simulated muscle forces. Extreme care was practiced to clamp the portion of the muscle that represented the resultant force direction of all muscle fibers. For the VM and VL, this was the distal portion of the muscle as it inserted into the patellar tendon and retinaculum. The VI was symmetrically trimmed to simulate a resultant force vector along the distal axis of the femur. The muscle clamps used in this study were made of stainless steel and were 8.0 cm × 3.0 cm × 0.8 cm. The clamp for the ITB was 6.0 cm × 2.5 cm × 0.8 cm.
We used a clamp, cable, and pulley system to apply loads to the individual muscles. The tendons were clamped to ensure even loading of all muscle fibers. Before clamping, we wrapped the muscles in saline moistened gauze to prevent drying during testing and to evenly distribute the force of the clamp through the tissue. The muscles were clamped as close to their respective tendinous insertions as possible, so tendinous fibers could be incorporated within the clamp. The VI and RF were clamped together, since the direction of the resultant force vectors of these muscles, with respect to the patella, is similar. All the clamping was performed such that the muscle fibers were perpendicular to the clamp. This further ensured even loading of the muscle fibers.
Specimen Mounting
We positioned and secured both the tibia and femur inside steel cylinders using diaphyseal bolts and threaded locking pins. Each was centered within the cylinders such that the long axis of the cylinders represented the long axis of the bones in the sagittal plane. We did this by using a custom external guide for the femur and an intramedullary guide for the tibia specifically developed for the PFJ testing jig used in this study. In addition, the femur was positioned within the proximal cylinder so that the cadaveric Q angle in the frontal plane was maintained. In this study, we defined and determined the cadaveric Q angle as the angle formed by the proximal tibial axis and the distal femur axis in the frontal plane with no external loads applied to the knee. This angle was measured with a standard goniometer with a precision of 0.5°.
We then mounted the knees in a custom knee jig machined out of aluminum to decrease spurious magnetic field interference. All additional hardware, such as screws, clamps, nuts, and bolts, was made from either stainless steel, aluminum, or plastic. The femur and tibia were positioned and fixed in their respective cylinders in its anatomic axial alignment with diaphyseal bolts and fixation screws. Then we mounted the knee joint to the custom PFJ testing jig. This custom knee jig provides 5° of freedom at the femur (3° translational, 2° rotational), and 3° of freedom at the tibia (3° rotational). This apparatus was fixed to a material testing machine frame (model 1122, Instron Corporation, Canton, MA), which was used to flex and extend the knee (Figure 1). A slotted aluminum plate (56 cm × 61 cm) attached to the back of the knee jig was used to mount and position the pulleys in an anatomic orientation of the muscle fibers. These pulleys were adjustable over a large area so that the direction of force for each muscle could be accurately simulated regardless of specimen size.
Experimental Procedure
The neutral position for each individual intact specimen under static conditions was first determined as described in our previous studies [35,36]. This neutral anatomic position of the patella in the PFJ was defined for each specimen as the position that exhibited the least tension on the quadriceps tendon. This was also used as the loading direction of the RF/VI. The determination of this position is essential for accurately assessing contact areas and pressures for each individual specimen. For loading of the individual muscles, anatomically based multiplane loading of the quadriceps mechanism and ITB was used (VL 98 N, VI/RF 111 N, ITB 27 N, VM 67 N) [33,37]. These loads are subphysiologic maximum, but the distribution of forces was scaled based on the physiological muscle cross-sectional area reported by Wickiewicz et al. [34]. The force on the VM for the varying conditions was 0 percent: no load, 50 percent: 33.5 N, 75 percent: 50.3 N, 100 percent: 67 N, 125 percent: 84 N, and 150 percent: 100.5 N. An additional 27 N, based on the cross-sectional area of the tensor fascia lata, was loaded onto the ITB. This load was based on the physiological cross-sectional area of the tensor fascia lata. For muscle loading directions, we adjusted each pulley so that the force application represented the primary fiber direction and orientation. We determined the muscle loading directions by measuring the muscle fiber insertion angle to the patella before the dissection. This technique was used in previous studies performed in our laboratory [33,37]. The fiber orientation of the quadriceps musculature with respect to the distal axis of the femur was similar to that of the values reported by Lieb and Perry and as in our previous studies [33,37,38]. The experiment consisted of two parts: the measurement of patellofemoral contact pressures and areas and the measurement of changes in the position of the patella in reference to the center of the epicondylar axis of the femur for varying simulated VM force changes. We collected the data at knee flexion angles of 0°, 30°, 60°, and 90°. In each condition, all the muscles were loaded simultaneously.

Figure 1. – PFJ testing jig.
PFJ Contact Area and Pressure Measurements
We measured the contact area and pressure using prescale (super-low) pressure-sensitive film (Fuji Photo Film Company, Tokyo, Japan) with a pressure range of 0.33 MPa to 2.94 MPa. Strips of film (4.0 cm × 5.0 cm) were placed in a polyethylene envelope and positioned within the joint through the suprapatellar pouch [33, 35–37]. The placement of the Fuji film in a polyethylene envelope was necessary for use in a fully lubricated joint. The total thickness of the Fuji film in the polyethylene envelope was 250 µm, and this has been shown to have a negligible effect on the measurement of contact pressures and areas in the diarth
roidal joint [39]. We obtained all measurements twice to ensure repeatability. In addition, films with any evidence of crinkling artifact were discarded and the measurement was repeated.
We scanned and analyzed the exposed film images on a Hewlett Packard (Boise, ID) Scan Jet IIc Color Scanner using the National Institutes of Health (Bethesda, MD) Image Version 1.62 program and the calibrated scale from the manufacturer. This program converted the Fuji film image into a scaled image with 256 levels of gray, which we used to determine the contact pressures and areas. The scanned images were analyzed for total contact area (mm2), peak contact pressure (MPa), and mean pressure (MPa). The peak pressure was defined as the average contact pressure of 5 percent of the total contact area with the highest contact pressure. The mean contact pressure was defined as the average contact pressure of the total contact area. Preliminary studies performed in our laboratory revealed the accuracy of the color scanner to be within 0.5 percent for area and pressure measurements [33,37]. The accuracy of Fuji film for absolute pressure measurement has been reported to be within 10 percent [40]. This absolute magnitude accuracy of the contact pressure measurements is the inherent limitation of the film, but in a comparative study such as in this study, the repeatability and reliability of the film are sufficient. Generally, the contact pressure measurement is underestimated.
Patellofemoral Joint Kinematic Measurements
A method for one to measure and analyze threedimensional (3-D) kinematic data for the PFJ using a system of magnetic tracking devices (Ascension Technology, Berlington, VT) was developed in our laboratory [41]. The benefit of this system is that we can monitor any arbitrary point in space, even a point in the interior of the bone itself, without the use of implanted markers by identifying external landmarks and correctly placing the magnetic receivers. This makes the process of tracking bone movements a relatively easy task once the tracking devices have been aligned and attached along the anatomic axes of the patella and the femur. The three translational motions are defined by a Cartesian coordinate system relative to the femur and the three rotational motions are described by Eulerian angles.
This magnetic tracking system consists of two tracking devices, which are called Birds, and their respective computer interface boxes, plus one magnetic field transmitter. The system is controlled by an IBM compatible personal computer (PC) with a Pentium microprocessor running Windows 95 operating system. Additional software used was Visual Basic 3.0 (Microsoft, Redmond, WA). We developed a custom application using Visual Basic, which implemented the necessary algorithms to track the movement of the patella and the femur in 3-D space. The system uses the anatomic femur axis and the epicondylar axis as the reference frame. Through the use of Eulerian angles and intersecting planes formed by the patella plane and femur axis, the kinematic relations of the PFJ can be measured without complicated setups, postdata processing, or explicit reference to an external reference frame, thus minimizing coordinate transformations and other complicated calculations. The Birds return measurements in 3-D space referenced to the internal reference frame as defined by the epicondylar and femoral axes.
After we mounted the knee onto the PFJ testing jig, the magnetic tracking device “Flock of Birds” was rigidly attached to the knee by stainless steel Steinmann pins and a Plexiglas holder. We inserted the Steinmann pin along the epicondylar axis of the femur using a custom drill guide specifically built for identification and drilling of the epicondylar axis. The “Bird” was then fixed to the Plexiglas holder with two Teflon screws. We were careful to ensure proper alignment of the receiver’s coordinate axis with the femoral axis and the epicondylar axis. The patella “Bird” was aligned and mounted along the anatomic axis of the patella. To do this, we carefully inserted a stainless steel Steinmann pin into the patella so as not to traverse the full thickness of the patella. For PFJ kinematic measurements, two receivers were used to establish Cartesian coordinate systems applied to the patella and distal femur (Figure 2(a)). The first receiver was fixed to the center of the anterior surface of the patella via a 1.5-mm stainless steel Steinmann pin into the bony cortex. The second receiver was secured to a 1.5-mm stainless steel Steinmann pin, which was placed along the epicondylar axis of the femur. The system software allowed 3-D measurement of the two receivers’ position relative to a global coordinate system projected by the magnetic transmitter.
Verification of Magnetic Tracking Device Performance with PFJ Testing Jig
We first determined the volume of space needed for the magnetic tracking sensors with the specimen mounted on to the PFJ testing jig (Figure 2(b)). This volume of space, which is spherical in shape and approximately 20 cm in diameter near the patella and the distal femur, is where the magnetic tracking sensors function to measure the PFJ kinematics. We then determined the accuracy and repeatability of the system in the testing environment by comparing the magnetic tracking device measurement to the Instron machine (Instron Company, Canton, MA, USA) output for the linear displacement (±0.001 mm) and a digital level (Pro Smart Level, Wedge Innovations, San Jose, CA, USA) (±0.1°) for the angular displacement. The accuracy in translation was within 0.34 mm, and the accuracy in rotation was within 0.5° for the volume of space where the magnetic tracking sensors function to measure the PFJ kinematics.
Statistical Analysis
We performed statistical analysis using analysis of variance (ANOVA). This analysis was repeated for each of the parameters, including knee flexion angle and VM strength. The level of significance was set at p = 0.05.
Results
The total contact pressures and areas for the simulated varying VM conditions in human cadaveric knees are shown in the Table. For patellofemoral contact pressures, an increase of 50 percent or a decrease of 100 percent in VM strength (150 percent VM and 0 percent VM condition, respectively) resulted in a statistically significant increase in pressure when all knee flexion angles were grouped together (p < 0.05) (Figure 3). With the 5 percent peak patellofemoral contact pressures, statistical significance was shown only when the VM strength was decreased by 100 percent (0 percent VM condition) and the knee flexion angles were grouped together (Figure 4). There was no statistically significant differences shown in the patellofemoral contact areas (p > 0.08). The patellar medial to lateral translation showed significance at 0 percent VM for 0°, 30°, 60°, and 90° of knee flexion (p < 0.05). In addition, a statistical significance was shown at 50 percent VM and also at 150 percent VM for 30° and 60° of knee flexion (p < 0.05) (Figure 5). The anterior to posterior translation across all knee flexion angles, showed no statistical significance with respect to VM strength variation (p > 0.05). The superior to inferior translation showed significance at 0 percent VM for 0°, 60° of knee flexion. In addition, a statistical significance was shown for 50 percent VM and 150 percent VM for 30° of knee flexion (p > 0.05). There was no significance in superior to inferior translation at 90° of knee flexion (Figure 6).
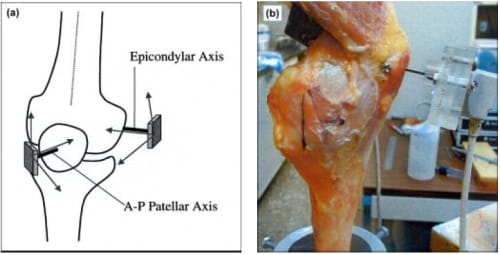
Figure 2. (a) Arrows show placement of stainless steel pins to measure patellar translations. (b) Magnetic tracking sensors mounted onto cadaveric knee.
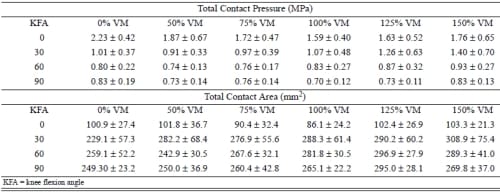
Table – Total PFJ contact pressures and areas for simulated VM strength conditions.
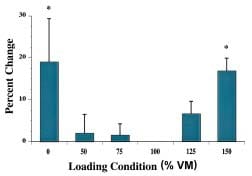
Figure 3 – Mean PFJ contact pressures with respect to VM strength variation. * indicates statistically significant difference compared to 100% VM.
Discussion
The findings from this human cadaveric study suggest that the isolated changes in VM strength in knees with loaded quadriceps may not significantly influence PFJ kinematics and PFJ contact pressures and areas. Patellofemoral contact pressures were significantly different from that with full VM force (100 percent VM) only when all the force was removed from the VM or if it was increased by 50 percent. Alteration in peak patellofemoral contact pressures also required complete removal of the VM force. Change in the kinematic data was heavily influenced by knee flexion angle. For example, with all force removed from the VM, the anterior to posterior translation was not different at 0° or 90°, but was at 30° and 60° of knee flexion. Overall, at least a 50 percent increase or decrease in VM force was required to demonstrate any change in patellar kinematics in the medial-lateral and superior-inferior direction.
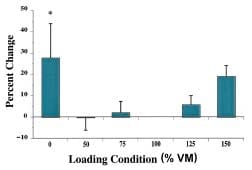
Figure 4 – Peak PFJ contact pressures with respect to VM strength variation. * indicates statistically significant difference compared to 100% VM.
Figure 5 – Medial patellar translation with respect to VM strength variation. * indicates statistically significant difference compared to 100% VM.
Figure 6 – Inferior patellar translation with respect to VM strength variation. * indicates statistically significant difference compared to 100% VM.
Although the position of the VM relative to other portions of the quadriceps seems advantageous for centering the patella, it remains controversial if selective strengthening of the VM is possible in vivo. Performing resisted hip adduction exercises, Hanten and Schulthies demonstrated selective VM activation, but its relevance to quadriceps muscle strengthening remains unknown [13]. An electromyographic study is complicated by low activity in both the VM and the VL during the last 30° of knee extension, when subluxation commonly occurs [42]. Mirzabeigi and coworkers studied the effects of hip rotation on selective VM and VL effort [6]. All four portions of the quadriceps muscle had electromyographic activity with isometric knee extension in neutral hip alignment. Yet, neither internal nor external rotation produced selective increase in effort of the VM relative to the VL. Results were similar for isokinetic exercises. Other investigators also failed to show selective increase in the VM effort and in fact demonstrated more activity in the VL, even at terminal knee extension [43,44]. Although selective endurance rehabilitation may be possible because of greater VM training effects relative to the VL, neither could be selectively activated with quadriceps muscle strengthening even when fatigued [45,46]. This study suggests that small decreases in the VM strength relative to the other portions of the quadriceps are unlikely to yield patellofemoral problems. Only VM rupture or complete paralysis would decrease the VM force comparable to all the force being removed from the VM. Both of these would require surgical intervention rather than rehabilitation. A prior study supported these findings. Lieb and Perry found that only a small force of 10 pounds on the VM was required to put the patella back into its neutral position in knee extension after 55 pounds of VL force had caused lateral patellar subluxation [38]. This suggests that even with the VL force imbalance of 45 pounds, the patella was maintaining its neutral position.
While cadaveric models have been effective for studying simulated muscle weakness, such models fail to recreate the synergy of joint stabilizing systems that are present in vivo. Joint proprioception contributes to stability, mediated by joint mechanoreceptors by initiating and coordinating muscle activity [47–49]. Cadaveric models also simplify complex muscle behavior as a single line of action from the centroid of the muscle to the tendon insertion [33]. In this study, the muscle forces were relatively low and the joint was loaded anatomically but statically. While this permitted accurate comparison of the loading conditions, it may be limited in demonstrating the effects of the knee muscle activities in PFJ stabilization.
Rehabilitation that included selective strengthening of the VM portion of the quadriceps muscle has been shown to be an effective treatment option for patellofemoral pain [50]. Treatment included iliotibial band stretching and patellar mobilizations that focused on stretching the lateral retinaculum. It may have been these latter treatments or strengthening of the quadriceps muscle as a whole that was responsible for the decrease in symptoms. Therefore, a clinical study addressing the issue of isolated VM strengthening and the PFJ is warranted.
Conclusion
In human cadaveric knees, the isolated changes in VM strength in knees with loaded quadriceps may not significantly influence PFJ kinematics and PFJ contact pressures and areas. Therefore, a clinical study addressing the issue of isolated VM strengthening and the PFJ is warranted.
References
- Ahmed AM, Burke DL, Hyder A. Force analysis of the patella mechanism. J Orthop Res 1987;5:69–85.
- Huberti HH, Hayes WC. Patellofemoral contact pressures: The influence of Q-angle and tendofemoral contact. J Bone Joint Surg 1984;66-A:715–24.
- Huberti HH, Hayes WC. Contact pressures in chondromalacia patellae and the effects of capsular reconstructive procedures. J Orthop Res 1988;6:499–508.
- Ahmed AM, Duncan, NA. Correlation of patellar tracking pattern with trochlear and retropatellar surface topographies. J Biomech Eng 2000;122(6):652–60.
- Chrisman OD. The role of articular cartilage in patellofemoral pain. Orthop Clin North Am 1986;17:231–34.
- Mirzabeigi E, Jordan C, Gronley JK, Rockowitz NL, Perry J. Isolation of the vastus medialis oblique muscle during exercise. Am J Sports Med 1999;27:50–53.
- Sandow MJ, Goodfellow JW. The natural history of anterior knee pain in adolescents. J Bone Joint Surg 1985; 67-B:36–38.
- Scuderi GR. Surgical treatment for patellar instability. Orthop Clin North Am 1992;23:619–30.
- Beim GM. Sports injuries in women. Womens Health 1999;2:27–34.
- Thomee R, Renstrom P, Karlsson J, Grimby G. Patellofemoral pain syndrome in young women. Scand J Med Sci Sports 1995;5:237–44.
- Fulkerson JP, Shea KP. Mechanical basis for patellofemoral pain and cartilage breakdown. In: Ewing JW, editor. Articular cartilage and knee joint function: Basic science and arthroscopy. New York: Raven Press; 1990. p. 93–101.
- Hvid I, Andersen L, Schmidt H. Chondromalacia patellae: The relation to abnormal patellofemoral joint mechanics. Acta Orthop Scand 1981;52:661–66.
- Hanten WP, Schulthies SS. Exercise effect on electromyographic activity of the vastus medialis oblique and vastus lateralis muscles. Phys Ther 1990;70:561–65.
- Heh
ne HJ. Biomechanics of the patellofemoral joint and its clinical relevance. Clin Orthop 1990;258:73–85. - Doxey GE. Assessing quadriceps femoris muscle bulk with girth measurements in subjects with patellofemoral pain. J Orthop Sports Phys Ther 1987;9:177–83.
- Garrick JG. Anterior knee pain. Physician Sports Med 1989;17:75–84.
- Fulkerson JP. Patellofemoral disorders: evaluation and management. J Am Acad Orthop 1994;2:124–32.
- Baker CL. Lower extremity problems in female athletes. J Med Assoc Ga 1997;86:193–96.
- Galanty HL, Matthews C, Hergenroeder AC. Anterior knee pain in adolescents. Clin J Sports Med 1994;4:176–81.
- Zappala FG, Taffel CB, Scuderi GR. Rehabilitation of patellofemoral joint disorders. Orthop Clin North Am 1992;23:555–66.
- Papagelopoulos PJ, Sim FH. Patellofemoral pain syndrome: diagnosis and management. Orthopaedics 1997; 20:148–57.
- Tria AJ, Palumbo RC, Alicea JA. Conservative care for patellofemoral pain. Orthop Clin North Am 1992;23: 545–54.
- Laprade J, Culham E, Brouwer B. Comparison of five isometric exercises in the recruitment of the vastus medialis oblique in persons with and without patellofemoral pain syndrome. J Orthop Sports Phys Ther 1998;27:197–203.
- Cuddigan JHP. Quadriceps femoris strength. Rheumatol Rehabil 1973;12:77–83.
- Ellis MI, Seedhom BB, Wright V, Dowson D. An evaluation of the ratio between the tensions along the quadriceps tendon and the patellar ligament. Eng Med 1980;189–94.
- Perry J, Antonelli D, Ford W. Analysis of knee joint forces during flexed-knee stance. J Bone Joint Surg [Am] 1975;57: 961–67.
- Huberti HH, Hayes WC. Contact pressures in chondromalacia patellae and the effects of capsular reconstructive procedures. J Orthop Res 1988;6(4):499–508.
- Ahmed AM, Burke DL, Yu A. In-vitro measurement of static pressure distribution in synovial joints—Part 11: Retropatellar surface. J Biomech Eng 1983;105:226–36.
- Maquet P. Mechanics and osteoarthritis of the patellofemoral joint. Clin Orthop 1979;144:70–73.
- Garg A, Walker PS. Prediction of total knee motion using a three-dimensional computer graphics model. J Biomech 1990;23:45–58.
- Heegaard J, Leyvraz PF, Curnier A. Rakotomanana L, Huiskes R. The biomechanics of the human patella during passive knee flexion. J Biomech 1995 Nov 28(11):1265–79.
- Goh JCH, Lee PY, Bose K. A cadaver study of the function of the oblique part of vastus medialis. J Bone Joint Surg Br 1995;77:225–31.
- Powers CM, Lilley JC, Lee TQ. The effects of axial and multi-plane loading of the extensor mechanism on the patellofemoral joint. Clin Biomech 1998;13:616–24.
- Wickiewicz TL, Roy RR, Powell PL, Edgerton VR. Muscle architecture of the human lower limb. Clin Orthop 1983;179:275–83.
- Lee TQ, Anzel SH, Bennett KA, Pang D, Kim WC. The influence of fixed rotational deformities of the femur on the patellofemoral contact pressures in human cadaver knees. Clin Orthop 1994;302:69–74.
- Lee TQ Gerken AP, Glaser F, Kim WC, Anzel SH. Patellofemoral kinematics and contact pressures in total knee arthroplasty. Clin Orthop 1997;340:257–66.
- Glaser FE, Gorab R, Lee TQ. Edge loading of the patellar component in TKA. J Arthoplasty 1999;14:493–99.
- Lieb FJ, Perry J. Quadriceps function. An anatomical and mechanical study using amputated limbs. J Bone Joint Surg 1968;50A:1535–48.
- Ateshian GA, Kwak SD, Soslowski LJ, Mow VC. A stereophotogrammetric method for determining in-situ contact areas in diarthroidal joints: a comparison study. Adv Bioeng ASME 22:35–38.
- Hale JE, Brown TD. Contact stress gradient detection limits of pressensor film. J Biomech Eng 1992;114:352–57.
- Lee TQ, Chan R, Mao T, McMahon P. A novel method for measuring patellofemoral kinematics. Transactions of the 45th Annual Meeting of the Orthopaedic Research Society; 1999, 45:946.
- Reynolds L, Levin TA, Medelros JM, Adler NS, Hallum A. EMG activity of the vastus medialis oblique and the vastus lateralis in their role in patellar alignment. Am J Phys Med 1983;62:61–70.
- Knight KL, Martin JA, Londeree BR. EMG comparison of quadriceps femoris activity during knee extension and straight leg raises. Am J Phys Med 1979;58:57–67.
- Smillie IS. Injuries of the knee joint, third edition. Baltimore: Williams & Wilkins Company; 1962. p. 3–5.
- Kaljumae U, Hanninen O, Airaksinen O. Knee extensor fatigability and strength after bicycle ergometer training. Arch Phys Med Rehabil 1994;75:564–67.
- Grabiner MD, Koh TJ, Miller GF. Fatigue rates of vastus medialis oblique and vastus lateralis during static and dynamic knee extension. J Orthop Res 1991;9:391–97.
- Vangness CT, Ennis M, Taylor JG, Atkinson R. Neural anatomy of the glenohumeral ligaments, labrum, and subacromial bursa. J Arthosc Rel Res 1995;11(2):180–84.
- Lephart SM, Pincivero DM, Giraldo JL, Fu FH. The role of proprioception in the management and rehabilitation of athletic injuries. Am J Sports Med 1997;24:130–37.
- Warner JJP, Lephart S, Fu FH. Role of proprioception in pathoetiology of shoulder instability. Clin Orthop Rel Res 1996;330:35–39.
- Doucette SA, Goble M. The effect of exercise on patellar tracking in lateral patellar compression syndrome. Am J Sports Med 1992;20:434–40.
