

Article
Related Links
Mohammad M. Alhalki,* MS, Maury L. Hull,*†‡ PhD, and Stephen M. Howell,†§ LTC, MC, USAFR
from the *Biomedical Engineering Graduate Group and the †Department of Mechanical Engineering, University of California at Davis, and the §Clinical Investigation Facility, David Grant Medical Center, Travis Air Force Base, California
ABSTRACT
The goal of this study was to determine how well a medial meniscal allograft restores the normal contact mechanics of the medial tibial plateau at the time of implantation. We measured maximum pressure, mean pressure, and contact area of the intact human cadaveric knee, the knee after meniscectomy, the knee with the original meniscus removed and reimplanted as an autograft, and the knee with an allograft. Measurements were made using pressure-sensitive film in 10 specimens loaded in compression to 1000 N at 0° 15° 30°, and 45° of flexion. The autograft and the allograft were identically implanted by cementing bone plugs attached to the meniscal horns in anatomic transtibial tunnels and suturing the outer edge of the meniscus to the remnant of the original meniscus. A medial meniscal allograft did not consistently restore normal contact mechanics because the process of implantation and the degree of match between the original and allograft meniscus affected the immediate load-bearing performance of the transplant. However, the allograft did significantly reduce the contact pressure compared with the knee after meniscectomy. If the results from this study can be extrapolated to patients, then using an allograft to restore contact mechanics to normal may require improvements in surgical technique and graft selection.
To counsel a patient considering meniscal allograft transplantation, it would be helpful to know if the procedure prevents degenerative arthritis. The observations that a meniscal allograft heals and that some patients experience shortterm pain relief and an improvement in function have been used to measure success and justify the use of the procedure in selected patients.4,17,19 However, studies in animal models have shown that degenerative changes still occur even when the meniscal transplant has healed.8,10 Because degenerative arthritis in a human knee takes years to evolve, long-term outcome studies have not been completed.18
A short-term method for evaluating whether degenerative arthritis can be prevented would be to determine if the maximum pressure, mean pressure, and contact area (that is, the contact mechanics) of the medial tibia1 articular surface in an intact knee are restored by a medial meniscal allograft at the time of implantation. The method of implantation and the allograft selected by the tissue bank may affect the restoration of normal contact mechanics, and each can be evaluated using human cadaveric knees.1 Identifying how each factor affects the contact mechanics might be useful for developing a strategy to improve the initial and long-term mechanical performance of meniscal allografts.
In this study, we chose to evaluate the effect of implanting a meniscal allograft in the medial hemijoint instead of the lateral hemijoint for two reasons. First, the medial meniscus is torn more commonly than the lateral meniscus7 and hence it is more likely to be repaired. Second, the effect of a medial meniscal allograft on tibia1 contact mechanics has not been determined. Although it has been found that a lateral meniscal allograft causes a significant decrease in contact area and an increase in maximum pressure,13 the effect of a medial meniscal allograft may be different because the anatomy of the two compartments is different. Therefore, the purpose of this study was to determine how well a medial meniscal allograft restores the normal contact mechanics of the medial tibia1 articular surface at the time of implantation.
MATERIALS AND METHODS
Specimen Selection, Preparation, and Testing
Ten fresh-frozen, human, cadaveric knees were obtained from six men and four women with an average age of 70 years (range, 37 to 89). Anteroposterior and lateral roentgenograms (with a radiopaque marker to correct for magnification) and MRI scans were obtained of each knee. There was no evidence of osteophytes, chondrocalcinosis, articular wear, or meniscal tears. Copies of the roentgenograms of the specimens were sent to the tissue bank (Cryolife, Inc., Marietta, Georgia) to be used to select the medial meniscal allografts.
Knee specimens were prepared for testing by performing a medial osteotomy to allow removal and reimplantation of the lateral meniscus as an autograft. Before the autograft was harvested, the osteotomy was reassembled and specimens with the medial meniscus intact were subjected to 1000 N of compressive load at flexion angles of 0° 15° 30°, and 45° Contact pressure on the medial articular surface of the tibia was measured with pressure-sensitive film (Super-Low Range; C Itoh, New York, New York).14
After measuring the contact pressure with the intact meniscus, the osteotomy was disassembled and a complete meniscectomy was performed, in which the meniscus was harvested as an autograft with bone plugs attached to the anterior and posterior horns. Further details of the specimen preparation and testing protocol can be found in our previously published article.1
The average age of the cryopreserved medial meniscal allografts was 29 years (range, 16 to 44). On the day of implantation, each allograft was thawed in warm saline after storage at -2O°C. The bone blocks were shaped to create bone plugs that matched those attached to the anterior and posterior horns of the original meniscus. Two millimeters of the outer meniscal edge were sharply removed from the medial meniscal allograft so that it would match the autograft, from which the outer edge was removed when it was harvested.
Using the same protocol that was used for the intact knee, the tibia1 articular pressure was remeasured with the medial meniscus removed (total meniscectomy), the medial meniscus reimplanted (autograft), and with the medial meniscal allograft implanted. These three joint conditions were tested randomly. We used exactly the same technique for inserting and fixing the autograft and the allograft. The osteotomy was disassembled, the bone plugs attached to the anterior and posterior horns of the transplant were cemented into the original tunnels to ensure anatomic placement, and the outer edge of the meniscus was sutured to the remnant of the original meniscus using single, vertical loop stitches of a 2-0 (metric 3-0) Ethibond polyester, braided suture (Ethicon, Somerville, New Jersey) spaced 10 mm apart.15 The osteotomy was reassemble
d, the preconditioning cycle was repeated to seat the graft, and the pressure was measured.
Data Analysis
Calibration curves for each knee were generated as described in our previous article.1 For each knee, three con-tact variables-the maximum pressure, the mean pressure, and the contact area-were determined at 0°, 15°, 30°, and 45° of flexion for each of four knee conditions. The four knee conditions were the normal knee, the knee after meniscectomy, the knee with the autograft, and the knee with the allograft. The 12 film packets exposed at a specific flexion angle from all four joint conditions were scanned simultaneously for consistency and then calibrated as described in our previous article. 1 The average value for each contact variable was computed from the three calibrated images at each flexion angle for each specimen and joint condition.
The maximum pressure, mean pressure, and contact area were normalized (as per our previously cited article) because the contact mechanics of the intact knee varied between specimens. To determine whether there was any difference between the normalized maximum pressure, normalized mean pressure, and normalized contact area between the intact knee, the knee after meniscectomy, and the knee with the autograft and allograft, a repeated measures analysis of variance (RANOVA) model was used to reduce experimental error.12 The independent variables included two withinspecimen factors: the four joint conditions, and the four flexion angles. Where significant differences were indicated (P < 0.05) for the RANOVA, paired comparisons were made using Tukey’s method.
RESULTS
The normalized maximum pressure was significantly affected by the different joint conditions (Table 1). According to Tukey’s test, the average normalized maximum pressures in the knees with the autograft and the knees with the allograft were significantly greater than in the intact knee, indicating that neither the autograft nor the allograft restored maximum pressure to normal (Fig. 1). The average normalized maximum pressures of the autograft and allograft were not significantly different from each other, indicating that the surgical implantation was the primary source of the significant increase in maximum pressure from that in the intact knee. Compared with the intact knee, the increase in normalized maximum pressure averaged over the four flexion angles was 25% for the autograft and 17% for the allograft. However, the confidence intervals (95%) at each flexion angle were wider for the allograft than for the autograft, indicating that the allograft caused greater variability in the normalized maximum pressure. The normalized maximum pressure was significantly less for the knees with the autograft and the knees with the allograft than for the knees after meniscectomy (100%) (P < 0.05).
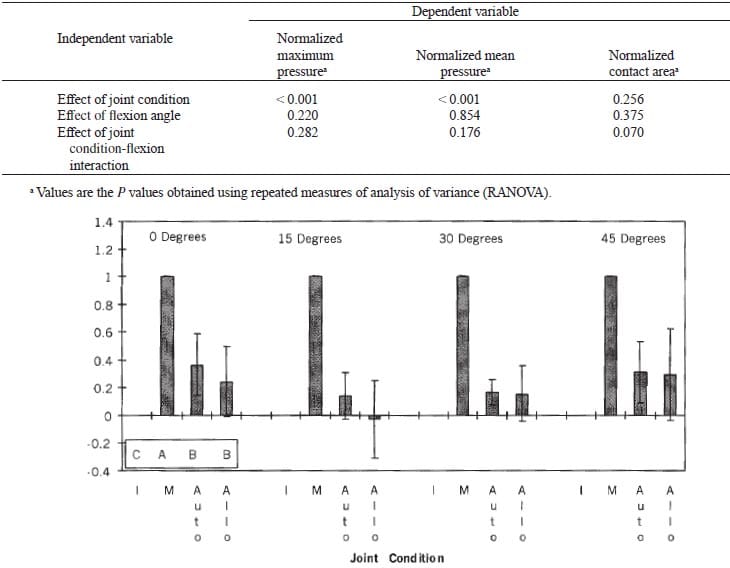
Figure 1. The normalized maximum pressure averaged over all of the specimens for the intact knee (I), the knee after meniscectomy (M), the knee with autograft (Auto), and the knee with allograft (Ailo) at four flexion angles. Shorter columns indicate a pressure closer to that of the normal knee. Error bars indicate 95% confidence limits. The normalized maximum pressure of the intact knee (C) was significantly less than that of the knee with the autograft (6) and allograft (6). The normalized maximum pressure in the knee after meniscectomy (A) was significantly greater than that in the intact knee (C) and the knee with the autograft (B) and allograft (B).
As with the normalized maximum pressure, the normalized mean pressure was significantly affected by the joint condition (Table 1). In contrast however, Tukey’s test showed that the normalized mean pressure in the knee with the autograft and in the knee with the allograft was not significantly different from that in the intact knee, indicating that both the autograft and allograft restored mean pressure close to normal (Fig. 2). Averaged over the four flexion angles, the normalized mean pressure increased 11% for the autograft, but decreased 5% for the allograft. As with maximum pressure, the confidence intervals (95%) of the normalized mean pressure at each flexion angle were wider for the allograft than for the autograft, indicating that the allograft caused greater variability in mean pressure. The normalized mean pressure was significantly less for both the knee with the autograft and the knee with the allograft than for the knee after meniscectomy (100%).
The normalized contact area in the knee with the autograft and in the knee with the allograft was not signif-icantly different from that of the intact knee (Table 1) because of the broad 95% confidence intervals for both the autograft and allograft joint conditions (Fig. 3). However, the normalized contact area in the knee with the allograft was less than that for the knee with the autograft, and comparable to the area in the knee after meniscectomy, at both 0’ and 15° of flexion. As the joint was flexed to 30° and 45°, however, the normalized contact area in the knee with the allograft was similar to that in the knee with the autograft but was still less than that in the normal knee.
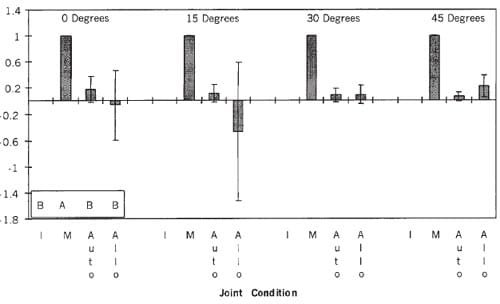
Figure 2. The normalized mean pressure averaged over all of the specimens for the four knee conditions (see abbreviations at the legend to Fig. 1) at four flexion angles. The normalized mean pressure of the intact knee (B) was not significantly different from that of the knee with the autograft (B) and allograft (B). The normalized mean pressure in the knee after meniscectomy (A) was significantly greater than in the other knee conditions. The confidence intervals of the normalized mean pressure of the knee with the allograft were wider than those for the autograft, indicating greater variability.
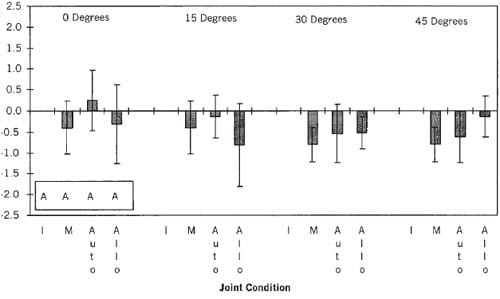
Figure 3. The normalized contact area averaged over all of the specimens for the four knee conditions (see abbreviations at the legend to Fig. 1 ) at four flexion angles. The normalized contact area of the intact knee (A) was not significantly different from that of the knee after meniscectomy (A) and the knee with the autograft (A) and allograft (A).
The primary difference in the three variables describing the contact mechanics between the autograft and allograft was the increase in variability associated with the use of the allograft. The impact of this variability can be illustrated by comparing the normalized mean pressure for three different specimens. In one specimen, the normalized mean pressure for the allograft was actually below that for the intact knee near full extension (Fig. 4A), in another specimen, the mean pressure was similar to that in the intact knee (Fig. 4B), and in another specimen the mean pressure was much greater than that in the intact knee (Fig. 4C). In all three examples the normalized maximum pressure with the autograft was consistently closer to normal compared with the allograft.
DISCUSSION
The three most important observations from this study were that 1) a medial meniscal allograft in a cadaveric knee did not restore normal contact mechanics of the medial tibia1 articular surface at the time of implantation, although 2) a knee with an allograft did reduce normalized maximum and mean contact pressures by 75% compared with a knee after meniscectomy, and 3) the contact mechanics in a knee with an allograft were more variable than in a knee with an autograft. Before discussing the clinical implications of these observations, several methodologic issues should be reviewed.</p >
Methodologic Issues
A discussion of the limitations associated with using pressure- sensitive film, the method of inserting, exposing, and removing the film from the knee, use of elderly knee specimens, and the load-application system for measuring tibia1 plateau contact mechanics has been detailed previously. 1,9 The consensus reached in these reports, and which also applies to this study, was that any limitations imposed by these sources did not affect the conclusions from the study.
It is unlikely that the structural properties of the osteoporotic bone of the elderly knee specimens changed during the study. The repetitive loading, which was limited to 1000 N, was only half of the compressive load in the knee during walking (1800 to 2000 N).11 Because the loads applied in our study were less than those in the act of walking, the application of these loads would not have been expected to change the structural properties of the knee. Furthermore, the order in which the knee conditions (after meniscectomy, with an autograft, and with an allograft) were tested was randomized. If any changes in structural properties did occur during testing, then the error would have been random. Although an increase in the random error would have inflated the variability in results, making it more difficult to detect statistically significant differences, the fact that many such differences were detected indicates that any increase in variability did not limit the usefulness of the study in drawing conclusions.
We used the best method for fixing a meniscal transplant so that we could determine whether either the autograft or allograft restored contact mechanics to normal at the time of implantation. Multiple studies have confirmed that tibia1 contact mechanics are closest to normal when bone attached to the anterior and posterior horns of the meniscus is fixed within transtibial bone tunnels or troughs.1,2,13 It has also been shown that the strongest peripheral suture repair relies on multiple, closely spaced (10-mm) vertical suture loops.15 Accordingly, both of these fixation methods were used to fix the autograft and the allograft. Bone cement was also used to reinforce and hold the osteoporotic bone plugs of the autograft. For experimental consistency, the stronger allograft bone plugs which were from younger donors) were cemented as well.
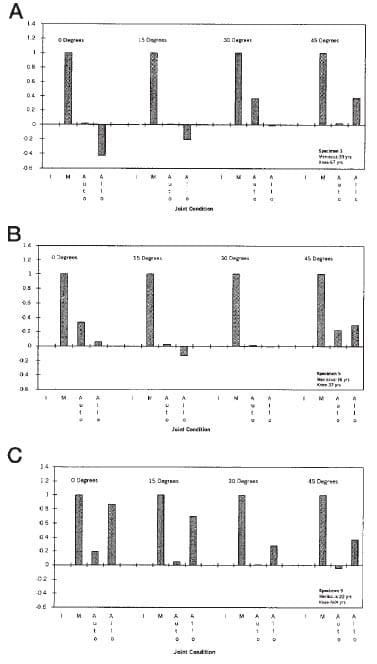
Figure 4. Normalized mean pressure for three different specimens. In specimen 3 (A), the normalized mean pressure for the allograft was actually below that of the intact knee near full extension. In specimen 5 (B), the mean pressure was similar to that of the intact knee. In specimen 9 (C), the mean pressure was much greater than that of the intact knee.
The technique of cementing bone plugs was different from the technique used in clinical practice, in which sutures are passed through the bone plugs and tunnels and tied over a bone bridge.16,20 The benefit from cementing the bone plugs was that the contact mechanics could be evaluated without the bone plug failing at physiologic loads.1 The contact mechanics with cementing the bone plugs provided a best-case analysis, and would have been either the same or better than the contact mechanics using suture fixation of bone plugs.
A femoral osteotomy was required to provide a complete exposure of the medial tibia1 plateau so that the autograft and allograft could be inserted anatomically. The contact mechanics of the medial tibia plateau as measured with pressure-sensitive film are the same before and after the femoral osteotomy.9 The excellent exposure allowed the drilling of two anatomically positioned transtibial bone tunnels by harvesting bone plugs attached to the anterior and posterior horns of the autograft using a core reamer.1 These two tunnels were then reused during the implantation of the autograft and allograft to ensure that both transplants were implanted anatomically. The use of the original bone tunnels eliminated the confounding variable (placement on the tibia1 plateau) that would have occurred if either the autografts or the allografts were inconsistently placed.
Although statistically significant increases were apparent in both the normalized maximum and mean pressures in the knee after meniscectomy, suggesting that the nor-malized contact area decreased, a suggestion that was confirmed from the contact-area measurements (Fig. 3), the statistical analyses failed to detect any significant differences in the contact area. Statistically significant differences in the normalized contact area were not detected because the contact area exhibited the largest variability,or widest confidence interval, of any of the three normalized dependent variables. The cause for this increased variability in the area measurement was small changes in the environmental conditions (temperature and humidity) that affect the sensitivity of the pressure-sensitive film. A previous study found that a change in temperature of 10°F and a change in relative humidity of 7% during the course of an experiment altered the contact area by 30%, while only minimally affecting the measurement of maximum pressure (7%) and mean pressure (12%).9
Interpretation and Significance of Results
Removing and reimplanting a medial meniscus as an autograft did not restore normal contact mechanics at the time of implantation. Compared with the intact knee, the normalized maximum pressure of the knee with an autograft was significantly greater (18%) and the normalized mean pressure was more variable. This deviation from normal contact mechanics was caused by the implantation procedure and was unavoidable even when the most secure currently available fixation method (cemented bone plugs and peripheral sutures) was used to reimplant the original meniscus.1
The keyhole technique, in which the bridge of bone left attached to both the anterior and posterior horns of the meniscal transplant is shaped like a keyhole in cross-section (technique developed by Arthrex, Inc., Naples, Florida) was not evaluated in this study for two reasons. At the time of the study, the keyhole technique was not used clinically for a medial meniscal transplant. Furthermore, using the keyhole technique to harvest and reinsert the medial meniscus as an autograft would have damaged the tibia1 plateau and affected the subsequent pressure measurements. Additional studies are required to determine whether the keyhole technique can improve the contact mechanics.
The contact mechanics with the allograft varied more from normal than did the contact mechanics with an autograft, indicating that the load-bearing capability of the allograft was different from that of the original meniscus, even though both grafts were implanted using the same fixation technique and transtibial tunnels. The larger variance from normal with the allograft compared with the autograft can be explained in part by the inability of the tissue bank to accurately match the three-dimensional geometry of the donor meniscus to the recipient knee.
The tissue bank’s selection of an allograft meniscus is based on a set of proprietary algebraic equations (Cryolife, Inc.) that relate transverse dimensions of the tibia1 plateau to the size of the medial meniscus. To provide input data to these equations, the tissue bank measured the maximum medial-lateral width and the maximum anterior- posterior depth of the medial compartment from AP and lateral roentgenograms of each cadaveric knee specimen and corrected these measurements for magnification. The tissue bank then selected the allograft on the basis of these two measurements made from the recipient’s knee. This method relies on the assump
tion that an allograft need match only the geometry in the transverse plane of the original meniscus to restore contact mechanics to the best degree possible within the limitations of fixation methods.
Mounting evidence suggests that this assumption for selecting an allograft is flawed because transverse geometry is not the only important determinant of tibia1 contact mechanics. This study and other clinical13 and experimental5 studies indicate that the cross-sectional geometry of the meniscus cannot be predicted by two roentgenographic measurements made in the transverse plane. Paletta et al.13 visually compared the peripheral height and radial depth of the original meniscus and a size-matched lateral meniscal allograft obtained from the same tissue bank that was used in our study. They noted gross differences in at least half the specimens and hypothesized that more careful matching of the cross-sectional shape might have improved the load-bearing performance of the lateral meniscal allograft. Haut et al.5,6 used a laser-based, digitized, three-dimensional coordinate system and observed that the cross-sectional shape of the medial and lateral menisci are only weakly predicted by measurements in the transverse plane.5 Therefore, compared with the autograft, the inferior load-bearing performance (greater variability) of the medial meniscal allograft in our study and of the lateral meniscal allograft in the study by Paletta et al. may have been caused by poor geometric match between the allograft and the original meniscus.
Differences in the material properties between the meniscal allograft and autograft could also explain why the contact mechanics in the knee with the allograft had greater variability from normal. At present, the selection procedure used by tissue banks involves no attempt to match material properties. This is understandable because the technology for making these measurements does not currently exist. However, inconsistent matching of material properties would be expected to introduce variability in the contact mechanics given the large variability between specimens in the key material properties such as the circumferential tensile modulus. 3.
Since neither geometry nor material properties of the allograft were matched to the original meniscus by the tissue bank, it is difficult to conclusively attribute the variability in the contact mechanics to either one factor or the other. Additional studies that quantify the variability introduced by each factor would be useful. Tissue banks could then use these findings to refine the selection procedure with the goal of providing a more closely matched meniscal allograft for the recipient’s knee. Considering the importance of matching allograft material properties and geometry in tibia1 contact mechanics, it is remarkable that the allografts used in this study restored contact mechanics compared with the intact knee as well as they did (Figs. 1 through 3).
Although neither the autograft nor the allograft meniscus restored normalized maximum pressure to normal, they both provided better load-bearing function than the knee after meniscectomy. The question that still needs to be answered is whether the significant decrease in normalized maximum pressure in the knee with the allograft compared with the knee after meniscectomy will either slow the rate or prevent the progression of osteoarthritis. This is difficult to answer, since to our knowledge no previous research has determined what relative increase in maximum pressure accelerates the rate of cartilage wear. Nevertheless, some perspective can be gained through two observations. One observation is that the increase in maximum pressure associated with the allograft still represents a significant reduction of more than 75% of the maximum pressure developed in the knee after meniscectomy. It is reasonable to assume that a reduction of this magnitude would reduce the rate of cartilage wear relative to the rate of cartilage wear in the knee after meniscectomy. Second, the finding that the mean pressure in both the knee after autograft and the knee after allograft was not significantly different from the mean pressure in the intact knee suggests that the maximum pressure was restricted to a relatively small region of the contact area. One can presume that high contact stresses developed over a large area would be more detrimental to the cartilage than locally high stresses, thus diminishing further the practical importance of the statistically significant increase in the normalized maximum pressure.
CONCLUSIONS
1. Because the process of implantation did not restore the original structural attachments of the meniscus to the surrounding tissues and because the allograft did not consistently match the original meniscus, a medial meniscal allograft in a cadaveric knee did not consistently restore normal contact mechanics at the time of implantation.
2. If the results from this cadaver study can be extrapolated to patients, then restoring contact mechanics to normal with an allograft may require improvements in surgical technique and graft selection (that is, matching size, shape, and material properties).
3. Even though the allograft did not match and was not secured as well as the intact meniscus, it still reduced the maximum and mean contact pressure by more than 75% compared with the knee after removal of the medial meniscus.
References
- Alhalki MM, Howell SM, Hull ML: How three methods for fixing a medial meniscal autograft affect tibial contact mechanics. Am J Sports Med 27: 320-328, 1999
- Chen Ml, Branch TP, Hutton WC: Is it important to secure the horns during lateral meniscal transplantation? A cadaveric study. Arthroscopy 1.2: 174- 181, 1996
- Fithian DC, Kelly MA, Mow VC: Material properties and structurefunction relationships in the menisci. Clin Orthop 252; 19-31, 1990
- Garrett JC: Meniscal transplantation, Am J Knee Surg 9: 32-34, 1996
- Haut TL, Hull ML, Howell SM: Use of roentgenography and MRI to predict meniscal geometry determined with a three dimensional coordinate digitizing system. J Orthop Res, in press, 2000
- Haut TL, Hull ML, Howell SM: A high-accuracy three-dimensional coordinate digitizing system for reconstructing the geometry of diarthrodial joints. J Biomech 31; 571-577, 1998
- Hede A, Larsen E, Sandberg H: Partial versus total meniscectomy: A prospective, randomized study with long-term follow-up. J Bone Joint Surg 746: 118-121, 1992
- Kuhn JE Wojtys EM: Allograft meniscus transplantation. Clin Sports Med 15: 537-556, 1996
- Martens TA, Hull ML, Howell SM: An in vitro osteotomy method to expose the medial compartment of the human knee, J Biomech Eng 119: 379- 385, 1997
- Mikic ZD, Brankov MZ, Tubic MV, et al: Transplantation of fresh-frozen menisci: An experimental study in dogs, Arthroscopy 13; 579-583, 1997
- Morrison JB: Function of the knee joint in various activities. Biomed Eng 4:573-580, 1969
- Neter J, Wasserman W, Kutner, MH: Applied Linear Statistical Models: Regression Analysis of Variance, and Experimental Designs. Third edition. Homewood, IL, Irwin, 1990
- Patetta GA Jr, Manning T, Snell E, et al: The effect of allograft meniscal replacement on intraarticular contact area and pressures in the human knee. A biomechanical study. Am J Sports Med 25: 692-698, 1997
- Pressure Measuring Fuji Prescale Film. Instructional Manual. Tokyo, Japan, Fuji Photo Film Co. Ltd., 1994
- Rimmer MG, Nawana NS, Keene GCR et al: Failure strengths of different meniscal suturing techniques. Arthroscopy 11: 146-150, 1995
- Shelton WR, Dukes AD: Meniscus replacement with bone anchors: A surgical technique [technical note]. Arthroscopy 10: 324-327, 1994.
- Van Arkel ERA, De Boer HH: Human meniscal transplantation. Preliminary results at 2 to 5-year follow-up. J Bone Joint Surg 77B: 589-595, 1995
- Veltri DM, Warren RF, Wickiewicz TL, et al: Current status of allograft meniscal transplantation. Clin Orthop 303: 44-55, 1994
- Verdonk R: Alternative treatments for meniscal injuries. J Bone Joint Surg 79B: 866-873, 1997
- Wilcox TR, Goble EM, Doucette SA: Goble technique of meniscus trans-plantation AM J Knee Surg 9: 37-42, 1996
