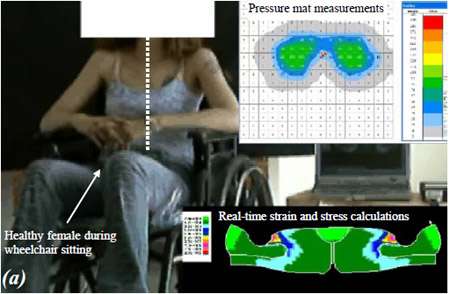
Eran Linder-Ganz (1), Ziva Yizhar (2), Amit Gefen (1) (1) Department of Biomedical Engineering Faculty of Engineering, Tel Aviv University Tel Aviv, ISRAEL (2) Department of Physical Therapy Faculty of Medicine, Tel Aviv University Tel Aviv, ISRAEL Introduction INTRODUCTION Deep pressure sores (DPS) under bony prominences in the buttock are a major concern for chronic wheelchair users, and injury is associated with excessive mechanical strains and stresses over critical time periods in deep muscles under the ischial tuberosities (IT) and sacrum [1]. Although several computational models were developed for simulation of strain/stress state under the IT during sitting, none of the published models is subject-specific or has the ability of real-time strain/stress analysis. Hence, none of the published models can be employed as a clinical tool for injury prevention. Moreover, in previous clinical studies that focused on pressure sore prevention, interface pressures between the patients’ buttocks and the cushions were measured and reported as a criterion for tissue injury, but the internal strains/stresses that actually caused the DPS are unknown. Accordingly, the goals of this study were (i) to develop a subjectspecific finite element (FE) model of the buttock that allows visualization and analysis of gluteal strains and stresses during wheelchair sitting in real-time, and (ii) to perform a small scale study in healthy subjects during wheelchair sitting to test the applicability of the above approach. Methods Subject-specific finite element modeling and validation A two-dimensional (2D), plane stress FE model of the IT and enveloping soft tissues (skeletal and smooth muscles, fat and skin) was developed based on a cross-sectional MRI anatomy. The FE code is clinically-oriented and, therefore, it is parametric and allows to define the dimensions of the bony prominences as well as the thickness and stiffness of the soft tissue layers to study their interactions in individuals. The IT-gluteus interface was set as “no-slip”, and sitting pressures, sampled at 10 Hz using a pressure mat (Tactilus, Sensor Products Co.), were fed into the model as real-time pressure boundary conditions (Figure). The FE system of equations is solved using the LU decomposition method. Briefly, this method provides the optimal time for solution in case that only the vector of boundary conditions is changing between multiple solutions [2,3]. To verify our real-time FE code for numerical accuracy, we compared its calculations with those of commercial FE software (Nastran 2004) and found differences that were smaller than 5 kPa. The subject-specific FE results were validated by comparing the predicted strains and stresses to muscle strains obtained from MRI images of subjects, and to muscle stresses obtained from physical phantom measurements, respectively. MR images were obtained for four healthy subjects (2 females and 2 males, age: 27-29, body weight: 55-85 Kg) before and during sitting, and subsequently, corresponding individual cross-sectional FE models were developed (using Nastran 2004) based on the unloaded MR images. Using a “reverse engineering” approach we fitted predicted deformed muscle contours (obtained from FE) to measured deformed muscle contours (obtained from MRI), separately for each subject, by adjusting fat viscoelastic moduli within a ±10% range. Then, intramuscular strains were calculated. Principal compression strains along vertical and horizontal paths in the transverse plane of muscles were compared. For each path, the cross-correlation between measured (MRI-based) and predicted (real-time FE-based) strains was calculated. We also calculated the means and standard deviations of errors for each path in each subject. A physical phantom of the buttock was also built, according to MRI scans through the pelvis of a seated female (age: 29 years, body weight: 54 Kg). The phantom contained a pelvic “bone” made of rigid plastic (E=12MPa, ν=0.3), and enveloping “soft tissues” made of silicone (E=1.6MPa, ν=0.49). Six ultra-thin flexible pressure sensors (FlexiForce, Tekscan Co.) were embedded in the phantom, under the IT to measure internal compressive stresses while the phantom is subjected to external loading. In addition, a pressure mat (Tactilus, Seonsor Product Co.) was located between the phantom and wheelchair to measure interface (“sitting”) pressures under the IT projections. The physical phantom was loaded with weights simulating 50 to 90 Kg body-weights in different positions: erect (90º) and nonerect (60º), right and left tilt (15º) and symmetrical loading. For each position, internal compressive stresses under the IT of the phantom and the corresponding sitting pressures were recorded simultaneously. Experimental Design Real-time, subject-specific FE models of the ischium region were built for the same four healthy subjects based on their MR images. Subjects were asked to sit in a wheelchair in a neutral position and watch a movie for 90 minutes (Figure). Based on continuous interface pressure measurements acquired using the pressure mat, real-time FE analysis of deep tissue strains and stresses in the buttocks was obtained for each subject (Figure). Specifically, we monitored peak principal compressive strains and peak principal compressive, shear and von Mises stresses in the right and left gluteus muscles (Table).  Real-time predictions of gluteal strains and stresses during wheelchair sitting using our subject-specific FE model: symmetrical sitting (above)
Real-time predictions of gluteal strains and stresses during wheelchair sitting using our subject-specific FE model: symmetrical sitting (above)
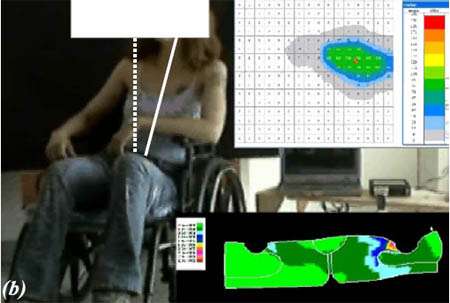
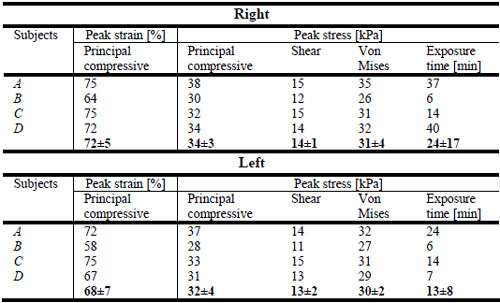
Real-time predictions of gluteal strains and stresses during wheelchair sitting using our subject-specific FE model: tilting to the left (above) Results For the four subjects, cross-correlations between deformed muscle contours calculated from MRI or using real-time FE did not drop below 0.8. The mean error between contours was smaller than 10%, and the standard deviation was kept below 5%. The internal stresses calculated using real-time FE were in very good agreement with internal stresses measured by the sensors embedded in the phantom (p>0.98). Mean value of the predictive error of the real-time FE model was found to be 4 ± 4 kPa (N=44 experiments). Our healthy subject studies showed maximal principal compressive strains of 72±5% and 68±7% in gluteus muscles under the right and left IT, respectively. Principal compressive, shear and von Mises stresses were found to be 34±3kPa, 14±1kPa and 31±4kPa under the right IT, and 32±4kPa, 13±2kPa and 30±2kPa under the left IT, respectively. Maximal continuous exposure to pressure was 24±17 min and 13±8 min for right and left sides, respectively (Table). Discussion In this study we developed a method and system that allow evaluation of deep tissue strains and stresses in real-time, in individual subjects. To test the applicability of this new approach, we calculated different strain/stress parameters in buttocks of four healthy subjects during prolonged wheelchair sitting. Interestingly, subject A who had the sharpest IT (radius of curvature of ~7 mm) showed the highest tissue strains and stresses in nearly all the parameters considered in the analysis (Table). It is therefore likely that sharpness of the IT has an important effect on internal tissue loading. It is also interesting that stress relieves differed substantially between subjects, e.g. subject B relived the gluteal stress more frequently (maximal exposure time of 6 min) than subject A (maximal exposure time of 37 and 24 min in right and left sides, respectively). Overall, we conclude that real-time FE is a valid method for monitoring gluteal and other deep tissue stress concentrations under the IT. We expect that the present method will make a substantial contribution to preventing severe DPS among chronic wheelchair users, including paraplegic, quadriplegic and geriatric patients. REFERENCES - Bouten, C. V., Oomens, C. W., Baaijens, F. P., and Bader, D. L., 2003, “The etiology of pressure ulcers: skin deep or muscle bound?” Arch Phys Med Rehabil, 84, pp. 616-619.
- Portnoy, S., Yarnitzky, G., Linder-Ganz, E., Yizhar, Z., and Gefen, A., 2005, “Real-time monitoring of internal loads in a residual limb during prosthetic gait: Verification and phantom results,” Salford’s 3rd International Conference on the Biomechanics of the Lower Limb in Health, Disease and Rehabilitation, Salford, UK, pp. 140-141.
- Yarnitzky, G., Yizhar, Z., and Gefen, A., 2005, “Real-time subjectspecific monitoring of internal deformations and stresses in the soft tissues of the foot: A new approach in gait analysis,” J Biomech, In Press.
|