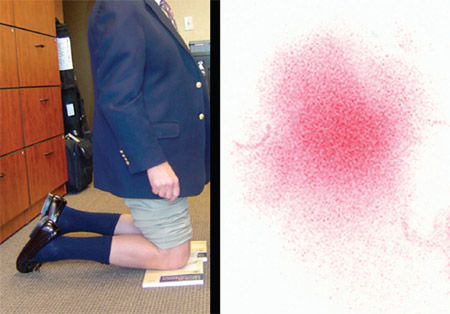
By Wayne M. Goldstein, MD, Alexander C. Gordon, MD, Jill Jasperson Branson, RN, BSN, Chris Simmons, BS, and Kimberly A. Berland, CST, FA Disclosure: The authors did not receive any outside funding or grants in support of their research for or preparation of this work. One or more of the authors or a member of his or her immediate family received, in any one year, payments or other benefits in excess of $10,000 or a commitment or agreement to provide such benefits from a commercial entity (royalties, DePuy). Also, a commercial entity (DePuy) paid or directed in any one year, or agreed to pay or direct, benefits in excess of $10,000 to a research fund, foundation, division, center, clinical practice, or other charitable or nonprofit organization with which one or more of the authors, or a member of his or her immediate family, is affiliated or associated. Introduction Many patients inquire if they will be able to kneel after total knee arthroplasty. We have cautioned patients regarding issues related to the patella that are associated with kneeling, yet, despite discomfort, many continue to kneel during various activities around the home or for religious reasons. While new high-flexion knee implant designs allow patients to get lower to the ground, the acts of cleaning a floor, gardening, exercising, and kneeling in prayer require bending down on both knees, and patients often state that they cannot kneel after total knee arthroplasty because of pain or that they do not attempt to kneel because the position feels awkward. Kneeling is part of daily life in certain cultures and, as elderly patients are more active, it is becoming an activity of increasing interest. Kneeling can be divided into three positions: kneeling at < 90° (for example, while praying on a riser in a place of worship), kneeling at 90° (for example, while gardening or scrubbing a floor), and kneeling at full flexion (for example, while praying on the floor). Several studies1,2 have evaluated mechanical foot stresses to improve footwear design and comfort. The Apex Harris Mat (Aetrex, Teaneck, New Jersey) captures a dynamic pressure print of the foot, with areas of highest pressure clearly identified. When a load is applied to the mat, ink will be deposited at the locations of highest pressure because all layers of the mat are compressed by the applied load. This information can be used to prevent harmful in-shoe conditions and can allow clinicians to provide better health care for patients with peripheral neuropathies1. We applied this technology to healthy volunteers and patients to determine high-stress areas during kneeling and created a pressure imprint of the knee that we called a kneelprint. We hypothesized that the location of the total knee arthroplasty incision might be a major contributor to discomfort during kneeling, so we modified the incision to avoid areas of kneeling stress and determined if this location resulted in more comfort for patients who desire to kneel. Materials and Methods Initially, a negative image was created by applying a wet stain to the knee of a healthy volunteer prior to kneeling. This image demonstrated the exact areas that would require mapping (Fig. 1). Ten healthy volunteers and one patient who had had a total knee arthroplasty one year previously were asked to kneel down on an Apex Harris Mat (Aetrex)3 with simultaneous pressure applied to both knees (Fig. 2). This imprinter produced a weight-bearing image of the anterior aspect of the knee (kneelprint), thereby demonstrating pressuredisbursement points. An additional institutional review board-approved study included a prospective sample of twenty-five healthy volunteers (fifty knees) (nine of whom also had the Harris mapping), four patients who had undergone total knee arthroplasty one to three years previously, and one patient who was evaluated both before and after total knee arthroplasty, all of whom were asked to kneel down with assistance on Pressurex Ultra Low (28-85 PSI) tactile pressure-indicating film (Sensor Products, Madison, New Jersey) that was placed on a consistent hard-floor surface (Fig. 3). Each participant was asked to face forward and upright without using hand support for nine seconds. One knee at a time was measured at each trial. Temperature, time, and humidity were recorded for each trial and were entered into the Topaq Pressure Analysis System flatbed scanner (Sensor Products) for analysis.  Fig. 1 Negative image of the pressure points created at the patella and tibia during kneeling by a healthy female volunteer. Fig. 1 Negative image of the pressure points created at the patella and tibia during kneeling by a healthy female volunteer. Fig. 2 Single kneelprint image (right) created on an Apex Harris Mat by a healthy male volunteer (left). Fig. 3 Single kneelprint image (right) created on pressure-indicating film by a male patient (left) after total knee arthroplasty. Nine of the healthy volunteers who were evaluated with the Apex Harris Mat were also evaluated with Pressurex Ultra Low (28-85 PSI) tactile pressure-indicating film (Fig. 4). Fig. 4 Pressure-indicating-film pseudocolor images (left) and three-dimensional-contour images (right) created at the patella and tibia during kneeling by a healthy female volunteer. Radiographs of the knees of one male patient were made three months after bilateral total knee arthroplasty to evaluate kneeling (Fig. 5). Fig. 5 Radiographs of the knees of a male patient, made with the patient kneeling on a thick pad three months after bilateral total knee arthroplasty. In May 2006, the senior author (W.M.G.) modified his traditional midline total knee arthroplasty incision by moving it medially to avoid pressure areas identified during the kneeling process. By the end of 2006, this surgeon had performed this incision during the treatment of 281 consecutive knees in non-obese patients. The incision started 2 to 3 cm medial to the tip of the tibial tubercle, lined up just medial to the medial edge of the patella. At the top of the patella, the incision was gradually angled laterally toward the quadriceps tendon. The incision was lengthened along the midline if excessive tension was observed in the skin. The capsular incision was made along this same path. At the top of the patella, a 5- mm cuff of quadriceps tendon was created and the incision was extended 1 to 2 cm and then into the vastus medialis. The patella was everted, and the knee was flexed (Fig. 6). Fig. 6 Illustration depicting the traditional midline total knee arthroplasty incision (left, green) and new medial midline incision (right, blue). (Reprinted, with permission, from Primal Pictures Ltd., London, United Kingdom.) Results Both the Apex Harris Mat and the pressure-indicating film usually identified two distinct areas of high stress on the kneelprint. One was located over the tibial tuberosity, and the other was located over the middle of the patella. The intensity of the stress most often varied over the tuberosity, where the presence of more body fat or rotation of the leg changed its location or intensity (Fig. 7). Fig. 7 Patellar (top) and tibial tuberosity (bottom) images made on Harris foot map (left) and pressure-indicating film (right) during the evaluation of a healthy female volunteer. Postoperative assessment of the total knee replacements revealed that all implants were within an acceptable range of alignment, with the femoral component in 5° to 7° of valgus and the tibial component at 90° to the long axis of the tibia. Pressure-film evaluation revealed the two distinct areas of stress in most knees, but some knees had no pressure points; this lack of pressure points appeared to be caused by fat distribution throughout the kneeling areas, particularly in obese patients who tended to have large fat deposits medially or a bulging intra-articular fat pad. In thin patients, the tibial tuberosity and the proximal crest of the tibia were consistently most prominent. As the patient or healthy volunteer leaned forward, distinct areas of pressure over the patella developed. When the total knee arthroplasty incision was located more medially (Fig. 8), most patients found little discomfort when kneeling one year after surgery. Fig. 8 Photographs showing healed medial midline incisions. Discussion Published studies have indicated that many patients cannot attempt or do not feel comfortable attempting to kneel because they are worried that kneeling will cause injury3-7. Palmer et al. studied seventy-five patients (100 knees) at least six months after surgery4. The investigators asked patients to comment on and demonstrate kneeling. Sixty-four knees were in patients who were able to kneel without discomfort or with mild discomfort, and twelve of the remaining knees were in patients who were unable to kneel because of problems not related to the knee. Twenty-four knees were in patients who were unable to kneel because of discomfort in the knee. There was no difference between the two groups with regard to overall knee scores, range of movement, and the presence of patellar resurfacing. Schai et al. questioned patients about their ability to kneel and their perception of factors affecting this ability after total knee arthroplasty8. Seventy patients (100 knees) were asked to comment on their ability to kneel. The investigators found that the patients’ perceived ability to kneel after total knee arthroplasty was less than their observed ability. In patients who had observed difficulty in kneeling, scar pain and back-related problems seemed to be the major limitations. Hassaballa et al. studied 253 knees that were treated with total, unicompartmental, or patellofemoral knee replacement knees were usually tender to palpation over the tuberosity. With the medial incision, most patients did not complain of pain on kneeling and did not have tenderness over the tibial tuberosity. Pain with kneeling may also be attributed to factors other than the incision. If there is flexion instability with posterior subluxation, kneeling may cause pain as the tibia is forced posteriorly and the femur moves anteriorly. This was unlikely in our patients because of the congruency of the components and the substantial lip of the tibial component (Fig. 5). Pain may also be caused by the host patella flexing over the component. This happens if the resection has been too aggressive, leaving a thin, flexible host patella. Danger to the patellar prosthesis during kneeling requires additional study. There are potential issues related to patellar loosening or host-bone fracture that have not yet been elucidated. Because kneeling is likely to be an intermittent activity, we will continue to accommodate the desires of our patients and perform the medial midline incision, placing it medial to the highest stress points documented in the kneeling pressure studies. Corresponding author: Jill Jasperson Branson, RN, BSN Illinois Bone and Joint Institute, 9000 Waukegan Road, Morton Grove, IL 60053 References - Bureau of Primary Health Care, Health Resources and Services Administration, United States Department of Health and Human Services. Pressure studies. https://bphc.hrsa.gov/nhdp/Pressure_Studies_RR.htm. Accessed 2006 Jun 7.
- Ralphs G, Lunsford TR, Greenfield J. Measurement of plantar pressure using fuji prescale film—preliminary study. J Prosthet Orthot. 1990;2:130.
- Weiss JM, Noble PC, Conditt MA, Kohl HW, Roberts S, Cook KF, Gordon MJ, Mathis KB. What functional activities are important to patients with knee replacements? Clin Orthop Relat Res. 2002;404:172-88.
- Palmer SH, Servant CT, Maguire J, Parish EN, Cross MJ. Ability to kneel after total knee replacement. J Bone Joint Surg Br. 2002;84:220-2.
- Hemmerich A, Brown H, Smith S, Marthandam SS, Wyss UP. Hip, knee, and ankle kinematics of high range of motion activities of daily living. J Orthop Res. 2006;24:770-81.
- Incavo SJ, Mullins ER, Coughlin KM, Banks S, Banks A, Beynnon BD. Tibiofemoral kinematic analysis of kneeling after total knee arthroplasty. J Arthroplasty. 2004;19:906-10.
- Nakagawa S, Kadoya Y, Kobayashi A, Tatsumi I, Nishida N, Yamano Y. Kinematics of the patella in deep flexion. Analysis with magnetic resonance imaging. J Bone Joint Surg Am. 2003;85:1238-42.
- Schai P, Gibbon AJ, Scott RD. Kneeling ability after total knee arthroplasty. Perception and reality. Clin Orthop Relat Res. 1999;367:195-200.
- Hassaballa MA, Porteous AJ, Newman JH, Rogers CA. Can knees kneel? Kneeling ability after total, unicompartmental and patellofemoral knee arthroplasty. Knee. 2003;10:155-60.
- Hassaballa MA, Porteous AJ, Newman JH. Observed kneeling ability after total, unicompartmental and patellofemoral knee arthroplasty: perception versus reality. Knee Surg Sports Traumatol Arthrosc. 2004;12:136-9.
- Horner G, Dellon AL. Innervation of the human knee joint and implications for surgery. Clin Orthop Relat Res. 1994;301:221-6.
|


 and three-dimensional-contour images (right)")


 and tibial tuberosity (bottom) images made on Harris foot map")

