

Article
Related Links
Aya Maedaa; Kazuhisa Soejimab; Mikinori Ogurac; Haruhito Ohmurea; Kazumasa Sugiharad; Shouichi Miyawakie
a Assistant Professor, Field of Developmental Medicine, Health Research Course, Department of Orthodontics, Graduate School of Medical and Dental Sciences, Kagoshima University, Kagoshima, Japan.
b Assistant Professor, Department of Oral and Maxillofacial Surgery, Miyazaki Medical College, University of Miyazaki, Miyazaki, Japan.
c Director, Department of Orthodontics, Maxillofacial Unit, Oita Oka Hospital, Oita, Japan.
d Professor and Department Chair, Maxillofacial Diagnostic and Surgical Sciences, Graduate School of Medical and Dental Sciences, Kagoshima University, Kagoshima, Japan.
e Professor and Department Chair, Field of Developmental Medicine, Health Research Course, Department of Orthodontics, Graduate School of Medical and Dental Sciences, Kagoshima University, Kagoshima, Japan.
Abstract
We performed an orthodontic treatment combined with mandibular distraction osteogenesis in a 15- year-old patient who wanted a correction of a chin deficiency and a protruding upper lip. The patient had an Angle Class II division 1 malocclusion with mandibular retrusion, a low mandibular plane angle, and scissors bite. First, a quad-helix appliance was applied to the mandibular dentition to correct the scissors bite in the bilateral premolar region. Later, a preadjusted edgewise appliance was applied to the maxillary and mandibular teeth. After 3 days, a mandibular distraction osteogenesis was performed. During and after the distraction, the open bite between the upper and lower dental arches was corrected using up and down elastics. The total treatment time with the edgewise appliance was 14 months. A skeletal Class I apical base relationship, good facial profile, and optimum intercuspation of the teeth were achieved with the treatment. The jaw-movement pattern on the frontal view did not change during gum chewing. However, the maximum gap without pain increased. The electromyographic (EMG) activity of the masseter and anterior temporalis muscles, and maximum occlusal force increased. The present case report suggests that an orthodontic treatment combined with mandibular distraction osteogenesis in a patient with mandibular retrusion in the late growth period might be effective for improving stomatognathic function.
Keywords: – Distraction; EMG; Occlusal force; Stomatognathic function
Introduction
In patients with skeletal Class II malocclusion and mandibular retrusion after a growth spurt, two alternative treatment methods are available; camouflage orthodontic treatment such as extraction case and surgical orthodontic treatment such as mandibular advancement surgery. Camouflage orthodontic treatment provides dental compensation without resolving the skeletal problem. Although mandibular advancement surgery is surgically invasive, it can resolve the skeletal disharmonies.1–6 Bilateral sagittal split osteotomy1–3 and mandibular distraction osteogenesis are frequently used as mandibular advancement surgeries.4–6
Mandibular advancement with a bilateral sagittal split osteotomy exceeding 7 mm is not recommended because postoperative skeletal relapse7–9 and condylar resorption10–12 often occur. When compared with the bilateral sagittal split osteotomy, mandibular advancement with a distraction osteogenesis exceeding 7 mm has several advantages: less postoperative skeletal relapse due to the relatively slow expansion of the soft tissue complex,13–15 less progressive condylar resorption,13–16 and less inferior alveolar nerve damage.17 Mandibular distraction osteogenesis is often applied to nonsyndromic patients who are 11–17 years old13 because of the high potential for bony regeneration.4–6,18 Mandibular distraction osteogenesis in particular was reported to be effective in patients with an average to low mandibular angle in a skeletal Class II malocclusion.19–21
It has been reported that patients with a mandibular retrusion show a low maximum electromyographic (EMG) activity and weak maximum occlusal force during clenching and mastication.22–25 Many reports have examined stomatognathic function after orthodontic treatment, including bilateral sagittal split osteotomy in patients with malocclusion.22,25,26–29 Some cases with skeletal Class II had improved stomatognathic function, 23,25 but other cases were unchanged or worse after orthognathic surgery.23,25,26 However, there have been few reports in which the changes of stomatognathic function were examined after mandibular distraction osteogenesis in patients with mandibular retrusion and Class II malocclusion. This article demonstrates the successful treatment of, and change in, the stomatognathic function after mandibular distraction osteogenesis in such a patient.
Case Report
Case Summary
The patient was a 15-year-old boy with a chief complaint of chin deficiency and protruding upper lip. No signs or symptoms of temporomandibular joint disorders (TMD) were noted.
His facial profile was a convex type with chin deficiency, a deep mentolabial sulcus, and protrusive upper lip (Figure 1a,b). The patient had an Angle Class II division 1 malocclusion with excessive overjet, a severe deep bite, scissors bite in the premolars, a lower constricted dental arch, and an upper spaced arch (Figure 2a–f).
The lateral cephalometric analysis indicated a skeletal Class II jaw relationship with an ANB angle of 7.0° and a severe short face with a mandibular plane angle of 12.0° and gonial angle of 107.5°. The maxillary incisor was protruded with a maxillary central incisor to the Frankfort plane angle (U1-FH angle) of 124.5°. According to the soft tissue analysis, lower facial height was short with subnasale-Gn of 59.5 mm and middle third height/lower third height (G-Sn/Sn-Me) of 1.2. A protruding upper lip was observed and the upper and lower lips were 5.0 mm ahead and 2.0 mm behind from the esthetic line (E-line), respectively (Figure 3A, Table 1). The mandibular growth spurt had passed according to the hand-wrist radiograph.
The jaw movement during gum chewing and EMG activity of the masseter and anterior temporalis muscles during clenching were examined by a 6 degreesof- freedom jaw movement and EMG recording system (Gnathohexagraph system, version 1.31, Ono Sokki, Kanagawa, Japan).30,35 The jaw movements of 20 cycles during chewing and masticatory muscle activity for 20 seconds during clenching were analyzed, respectively. If the jaw-movement trajectory in the opening phase was medial of that of the closing phase on the frontal view, the jaw-movement pattern was classified into the normal type.
Occlusal force and the occlusal contact area were also examined by an occlusal force recording system (Dental Prescale & Occluzer, Fuji Film, Tokyo, Japan).29,36 Around 90% of jaw movement during gum chewing was the normal type in the frontal view (Table 2). The maximum gap without pain was 44.2 mm. The EMG activity of the masseter and anterior temporalis muscles was low, maximum occlusal force was weak, and the occlusal contact area was narrow when compared with normal subjects26,37 (Figure 4, Table 2).
Diagnosis
This case was diagnosed as an Angle Class II division 1 malocclusion with low mandibular plane angle, skeletal Class II, mandibular retrusion, and scissors bite in the premolar region.
Treatment Plan
Treatment was planned as follows:
- Lengthening of the mandibular body by distraction osteogenesis to improve the mandibular retrusion;
- Expansion of the lower constricted dental arch to improve the scissors bite in the premolar region with lower constricted dental arch; and
- Retraction of the maxillary anterior teeth and aligning all teeth with preadjusted edgewise appliances to reduce the overjet and overbite.
Treatment Alternatives
In the patient with skeletal Class II malocclusion and mandibular retrusion after the growth spurt, the alternative treatment method is camouflage orthodontic treatment with extraction. However, this treatment does not resolve the skeletal problem. Therefore, we selected surgical orthodontic treatment because his chief complaint was chin deficiency and a protruding upper lip. Two surgical techniques are available, bilateral sagittal split osteotomy or mandibular distraction osteogenesis. We selected mandibular distraction osteogenesis since the amount of mandibular distraction needed was more than 7 mm.
Treatment Progress
The lower arch in the premolar region was expanded with a quad helix appliance for 5 months (at age 15 years 4 months) to correct the scissors bite. A preadjusted edgewise appliance (0.018 x 0.025 inch) was placed in the maxillary and mandibular arches 3 days before mandibular distraction osteogenesis. A mandibular distraction osteogenesis was performed using an intraoral distraction devise (KLS Martin, Umkirch, Germany) that was attached to the lower third molar area and the anterior border of the mandibular rami (at age 15 years 11 months). The device was activated on day 8 after surgery at a rate of 1 mm/day (0.5 mm every 12 hours). Activation was continued for 9 days so that the patient had an edge-toedge occlusion. At the end of the distraction period a lateral open bite was observed. Postsurgical orthodontic treatment such as leveling and alignment of the teeth was then performed (Figure 3B). Up and down elastics were used in the premolars area for 8 months during and after the distraction to prevent postoperative skeletal relapse and to improve the lateral open bite. Eight months after surgery, the distraction device was removed. After 14 months of edgewise treatment, a skeletal Class I apical base relationship, good facial profile, and optimum intercuspation of the teeth were achieved. The patient wore Begg-type and Hawleytype retainers all day for 1 year.
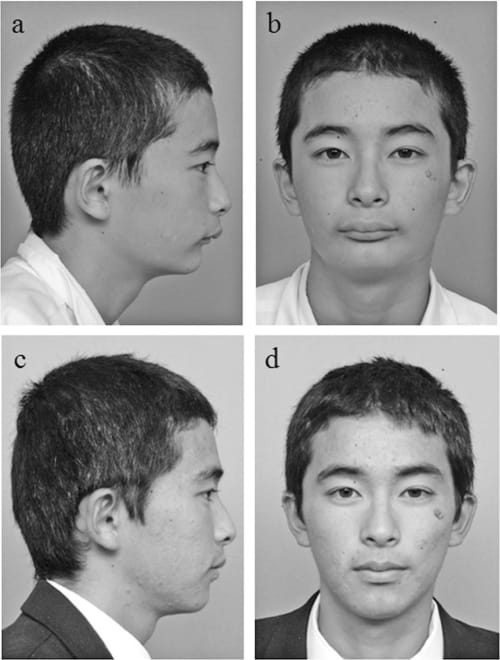
Figure 1. Facial photographs. (a and b) Pretreatment, age 15 years 0 months. (c and d) Posttreatment, age 17 years 1 month.
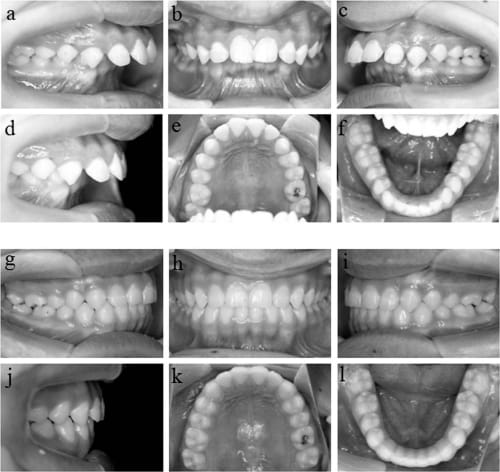
Figure 2. Pretreatment intraoral photographs. (a–f) Pretreatment, age 15 years 0 months. (g–l) Posttreatment, age 17 years 1 month.
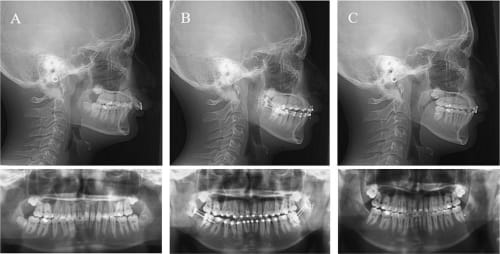
Figure 3. Lateral cephalographs and panoramic radiographs. (A) Pretreatment, age 15 years 0 months. (B) 1 month after mandibular distraction osteogenesis, age 16 years 0 months. (C) Posttreatment, age 17 years 1 month.
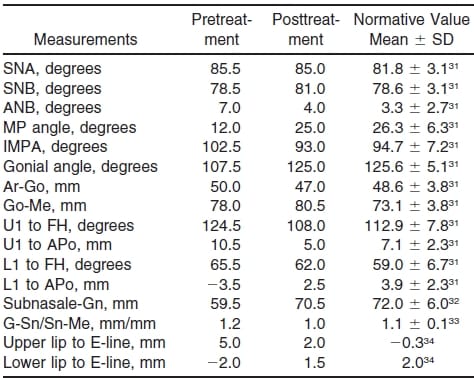
Table 1. Cephalometric Measurements
Results
At the end of treatment, the patient showed a good facial profile, a balanced lip line, and an acceptable occlusion. The chin deficiency, protruding lip, deep mentolabial sulcus, and protrusive upper lip were improved (Figure 1c,d). The scissors bite in the premolar region was also improved. The dental arches were aligned and leveled with an ideal overjet and overbite (Figure 2g–l). The lateral cephalometric analysis indicated a skeletal Class I apical base relationship with an ANB angle of 4.0° and balanced face with an average mandibular plane angle of 25.0° and a gonial angle of 125°. The mandible was advanced horizontally 3 mm and vertically 12 mm. The upper incisors were retruded with U1-FH angle of 108°. According to the soft tissue analysis, the lower facial height was in the normal range with a subnasale-Gn of 70.5 mm. A protruding upper lip and retracted lower lip were improved such that the upper and lower lips were 2.0 mm and 1.5 mm ahead of the E-line, respectively (Figures 3C and 5, Table 1).
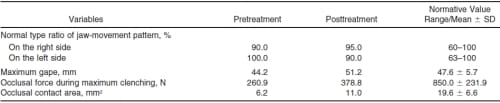
Table 2. Variables in the Stomatognathic Function

Figure 4. Masseter and temporalis muscle activity during clenching. (a) Right side. (b) Left side.
The jaw-movement pattern did not change on the frontal view during gum chewing. However, the maximum gap without pain improved from 44.2 mm to 51.2 mm. The masseter and anterior temporalis muscle activity, occlusal force, and occlusal contact area increased after treatment (Figure 4, Table 2).
Discussion
We performed an orthodontic treatment combined with mandibular distraction osteogenesis in a 15-yearold patient who wanted correction of his chin deficiency and a protruding upper lip. In the current case, the mandibular body length increased by 2.5 mm. The skeletal problem was improved and a good facial profile was achieved. The patient showed acceptable good occlusion and maximum interdigitation of the teeth due to the increase of the occlusal area after the treatment. The maximum gap without pain, masticatory muscle activity, and occlusal force increased after orthodontic treatment combined with mandibular distraction osteogenesis. The increase in the maximum gap after treatment may be due to lengthening of the mandibular body by distraction osteogenesis.
In this case, the EMG activity of the masseter and anterior temporalis muscles and occlusal force at pretreatment were very low because the occlusal contact area was narrow. With regard to the increases in muscle activity and occlusal force, previous reports suggested close relationships between the masticatory muscle activity, occlusal force, and occlusal contact area.38,39 Therefore, the increase in occlusal contact area after treatment may have contributed to the increase in muscle activity and occlusal force.
There have been many reports that the stomatognathic function changed after mandibular advancement surgery by bilateral sagittal split osteotomy. 23–26,40,41 Some cases with skeletal Class II showed an increase in maximum occlusal force or the masseter and anterior temporalis muscle activity after orthognathic surgery.23,25,40 However, few cases with skeletal Class II had improved stomatognathic function after orthognathic surgery. Other cases showed unchanged or worsened function, eg, the masseter and anterior temporalis muscle activity or maximum occlusal force did not change25,26 or the occlusal force decreased23,41 after orthognathic surgery. However, to date, there have been few reports in which the changes of stomatognathic function were examined after mandibular distraction osteogenesis in patients with skeletal Class II.
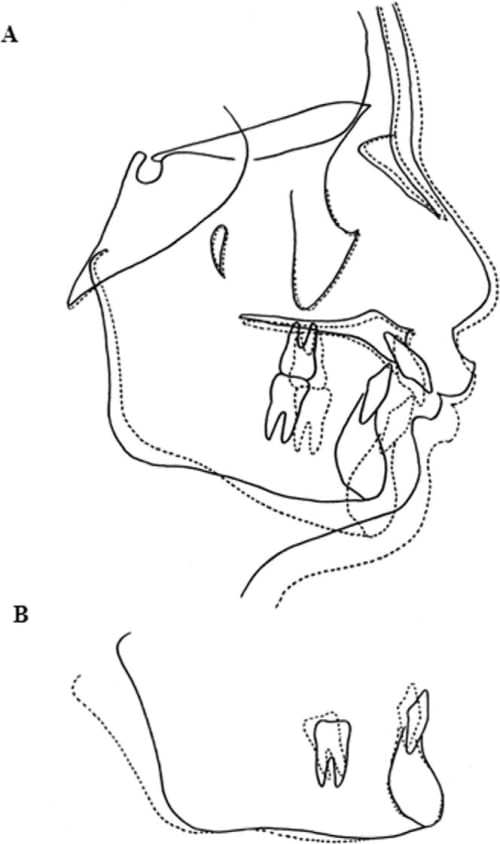
Figure 5. Superimposition of cephalometric tracings before (solid line) and after (dotted line) treatment. (A) A best-fit on the anterior wall of sella turcica, the greater wings of the sphenoid, the cribriform plate, the orbital roofs, and the surface of frontal bone. (B) A bestfit on the mandibular plane at Me.
The present case showed improvement of stomatognathic function and no signs or symptoms of TMD after orthodontic treatment combined with mandibular distraction osteogenesis. Therefore, it was suggested that surgical orthodontic treatment with mandibular distraction osteogenesis was effective in resolving the skeletal disharmonies, and improving the facial profile, occlusion, and stomatognathic function.
Conclusion
Surgical orthodontic treatment combined with mandibular distraction osteogenesis may be an effective method for improving occlusion, facial profile, and stomatognathic function.
References
- Trauner R, Obwegeser H. The surgical correction of mandibular prognathism and retrognathia with consideration of genioplasty. Part I. Surgical procedures to correct mandibular prognathism and reshaping of the chin. J Oral Surg. 1957;10:677–689.
- Grammer FC, Carpenter AM. A quantitative histologic study of tissue responses to ramal sagittal splitting procedures. J Oral Surg. 1979;37:482–485.
- Wyatt WM. Sagittal ramus split osteotomy: literature review and suggested modification of the technique. Br J Oral Maxillofac Surg. 1997;35:137–141.
- Tavakoli K, Stewart KJ, Poole MD. Distraction osteogenesis in craniofacial surgery: a review. Ann Plast Surg. 1998;40: 88–99.
- van Strijen PJ, Perdijk BT, Breuning KH. Distractie-osteogenese. Een nieuwe ontwikkeling in de aangezichtschirurgie. Ned Tijdschr Tandheelkd. 1998;105:129–131.
- McCarthy JG, Stelnicki EJ, Mehrara BJ, Longaker MT. Distraction osteogenesis of the craniofacial skeleton. Plast Reconstr Surg. 2001;107:1812–1827.
- van Sickels JE, Richardson DA. Stability of orthognathic surgery: a review of rigid fixation. Br J Oral Maxillofac Surg. 1996;34:279–285.
- Mobarak KA, Espeland L, Krogstad O, Lyberg T. Mandibular advancement surgery in high-angle and low-angle Class II patients: different long-term responses. Am J Orthod Dentofacial Orthop. 2001;119:368–381.
- Dolce C, Hatch JP, Van Sickels JE, Rugh JD. Rigid versus wire fixation for mandibular advancement: skeletal and dental changes after 5 years. Am J Orthod Dentofacial Orthop. 2002;121:610–619.
- Moore KE, Gooris PJJ, Stoelinga PJW. The contributing role of condylar resorption to skeletal relapse following mandibular advancement surgery. J Oral Maxillofac Surg. 1991;49: 448–460.
- Arnett GW, Milam SB, Gottesman L. Progressive mandibular retrusion-idiopathic condylar resorption. Part 1. Am J Orthod Dentofacial Orthop. 1996;110:8–15.
- Hoppenreijs TJM, Stoelinga PJW, Grace KL, Robben CMG. Long-term evaluation of patients with progressive condylar resorption following orthognathic surgery. Int J Oral Maxillofac Surg. 1999;28:411–418.
- van Strijen PJ, Breuning KH, Becking AG, Tuinzing DB. Stability following distraction osteogenesis to lengthen the mandible: results in 50 patients. J Oral Maxillofac Surg. 2004; 62:304–307.
- Diner PA, Kollar EM, Martinez H, Vazquez MP. Intraoral distraction for mandibular lengthening: a technical innovation. J Craniomaxillofac Surg. 1996;24:92–95. 15. Tavakoli K, Stewart KJ, Poole MD. Distraction osteogenesis in craniofacial surgery: a review. Ann Plast Surg. 1998;40: 88–99.
- Thurmu¨ ller P, Troulis MJ, Rosenberg A, Kaban LB. Changes in the condyle and disc in response to distraction osteogenesis of the minipig mandible. J Oral Maxillofac Surg. 2002;60:1327–1333.
- Whitesides LM, Meyer RA. Effect of distraction osteogenesis on the severely hypoplastic mandible and inferior alveolar nerve function. J Oral Maxillofac Surg. 2004;62:292– 297.
- Hollier LH, Higuera S, Stal S, Taylor TD. Distraction rate and latency: factors in the outcome of pediatric mandibular distraction. Plast Reconstr Surg. 2006;117:2333–2336.
- Mommaerts MY, Jacobs W, de Jonghe N. Mandibular distraction using a dynamic osteosynthesis system: MD-DOS. Concepts and surgical technic [in French]. Rev Stomatol Chir Maxillofac. 1998;99:223–230.
- Karacay S, Akin E, Okcu KM, Bengi AO, Altug HA. Mandibular distraction with MD-DOS device. Angle Orthod. 2005; 75:685–693.
- Schreuder WH, Jansma J, Bierman MW, Vissink A. Distraction osteogenesis versus bilateral sagittal split osteotomy for advancement of the retrognathic mandible: a review of the literature. Int J Oral Maxillofac Surg. 2007;36:103– 110.
- Tate GS, Throckmorton GS, Ellis E III, Sinn DP. Masticatory performance, muscle activity, and occlusal force in preorthognathic surgery patients. J Oral Maxillofac Surg. 1994;52: 476–481.
- Throckmorton GS, Ellis E III, Sinn DP. Functional characteristics of retrognathic patients before and after mandibular advancement surgery. J Oral Maxillofac Surg. 1995;53: 898–908 ; discussion 908–909.
- Harper RP, de Bruin H, Burcea I. Muscle activity during mandibular movements in normal and mandibular retrognathic subjects. J Oral Maxillofac Surg. 1997;55:225–233.
- Zarrinkelk HM, Throckmorton GS, Ellis E III, Sinn DP. Functional and morphologic changes after combined maxillary intrusion and mandibular advancement surgery. J Oral Maxillofac Surg. 1996;54:828–837.
- van den Braber W, der Glas HW, van der Bilt A, Bosman F. Masticatory function in retrognathic patients, before and after mandibular advancement surgery. J Oral Maxillofac Surg. 2004;62:549–554.
- Miyawaki S, Takada K. Incisor crossbite and repaired unilateral cleft lip and palate: changes in jaw movement and temporalis muscle activity before and after edgewise treatment— case report. Cleft Palate J. 1997;34:533–537.
- Miyawaki S, Tanimoto Y, Araki Y, Katayama A, Kuboki T, Takano-Yamamoto T. Movement of the lateral and medial poles of the working condyle during mastication in patients with unilateral posterior crossbite. Am J Orthod Dentofacial Orthop. 2004;126:549–554.
- Miyawaki S, Araki Y, Tanimoto Y, Katayama A, Fujii A, Imai M, Takano-Yamamoto T. Occlusal force and condylar motion in patients with anterior open bite. J Dent Res. 2005; 84:133–137.
- Miyawakil S, Ohkochi N, Kawakami T, Sugimura M. Effect of food size on the movement of the mandibular first molars and condyles during deliberate unilateral mastication in humans. J Dent Res. 2000;79:1525–1531.
- Miyashita K. An Atlas of Roentgen Anatomy and Cephalometric Analysis. Tokyo, Japan: Quintessenz; 1986.
- Farkas LG. Anthropometry of the Head and Face in Medicine. New York, NY: Elsevier Science Publishing Co; 1981.
- Alcalde RE, Jinno T, Orsini MG, Sasaki A, Sugiyama RM, Matsumura T. Soft tissue cephalometric norms in Japanese adults. Am J Orthod Dentofacial Orthop. 2000;118:84–89.
- Asai Y. The evaluation of soft tissue profile by cephalometric X ray. In: Susami M, Nakago T, eds. The Series of Clinical Orthodontics. Vol 1. Tokyo, Japan: Ishigaku Co; 1976: 237–247.
- Miyawaki S, Ohkochi N, Kawakami T, Sugimura M. Changes in masticatory muscle activity according to food size in experimental human mastication. J Oral Rehabil. 2001;28: 778–784.
- Nakata Y, Ueda HM, Kato M, et al. Changes in stomatognathic function induced by orthognathic surgery in patients with mandibular prognathism. J Oral Maxillofac Surg. 2007; 65:444–451.
- Miyawaki S. Influence of occlusal contacts during chewing on masticatory function in preadolescents with repaired unilateral cleft lip and palate. J Osaka Univ Dent Sch. 1994; 39:96–122.
- Gurdsapsri W, Ai M, Baba K, Fueki K. Influence of clenching level on intercuspal contact area in various regions of the dental arch. J Oral Rehabil. 2000;27:239–244.
- Hidaka O, Iwasaki M, Saito M, Morimoto T. Influence of clenching intensity on bite force balance, occlusal contact area, and average bite pressure. J Dent Res. 1999;78: 1336–1344.
- Youssef RE, Throckmorton GS, Ellis E III, Sinn DP. Comparison of habitual masticatory cycles and muscle activity before and after orthognathic surgery. J Oral Maxillofac Surg. 1997;55:699–707.
- Proffit WR, Turvey TA, Fields HW, Phillips C. The effect of orthognathic surgery on occlusal force. J Oral Maxillofac Surg. 1989;47:457–463.
