

Article
Related Links
Etsuko Motegi, Mayumi Nomura, Chie Tachiki, Haruyo Miyazaki*, Fumie Takeuchi**, Sakiko Takaku, Yuriko Abe, Mariko Miyatani, Takahiro Ogai, Asuka Fuma, Hiroko Fukagawa*, Masataka Kano and Kenji Sueishi
Department of Orthodontics, Tokyo Dental College, 1-2-2 Masago, Mihama-ku, Chiba 261-8502, Japan
* Division of Orthodontics, Department of Oral Health Clinical Science, Tokyo Dental College, 2-9-18 Misaki-cho, Chiyoda-ku, Tokyo 101-0061, Japan
** Ogura Orthodontic Clinic, 2-19 Shinden-cho, Chuou-ku, Chiba 260-0027, Japan
Abstract
The “8020” goal of retaining 20 or more teeth after the age of 80 necessitates investigating oral health status in people below the age of 80. The purpose of this study was to determine similarities and differences between people in their sixties attending college and achievers of the 8020 goal. The results of oral examination and occlusal force measurement in 46 students enrolled at a college for the elderly in Chiba City with an average age of 66.9 years (22 men, 24 women) were compared with data from previous surveys of fifty-two 8020 achievers (28 men, 24 women). Occlusal force was measured and evaluated using Dental Prescale (Fuji Photo Film Co., Tokyo). The average number of present teeth was 25.8, and no subjects showed anterior crossbite, comparable with findings in 8020 achievers. Average occlusal force was 942.9±440.1 N (1,029.6±545.9 N for men, 863.4±305.1 N for women), not significantly different from that in 8020 achievers. The results of multiple regression analysis suggest that occlusal force is unaffected by aging if many teeth are present.
Key words: Occlusal force—Sixties—College for the elderly—Normal occlusion— 8020
Introduction
The 2005 Ministry of Health, Labour and Welfare (MHLW) dental health survey revealed that people of 80 years of age had an average of 10 present teeth, with 20% achieving the goal of the Japanese dental health “8020” campaign aimed at the retention of 20 or more teeth at age 80 and over. It is necessary to carry out oral health promotions and surveys targeting people under the age of 80. Ueno et al.19) conducted a study on the number of present natural teeth and functional tooth units in 2,164 Japanese aged 40 to 75 years by means of a questionnaire and oral examination to determine decrease in total number of present teeth and functional tooth units with age. Total-functional units, which were defined as pairs of opposing natural teeth and artificial teeth in the 50–59-year age group, was slightly lower compared with that in other age groups. Hugo et al.7) investigated physical and psychological dimensions of QOL, including bite force, in 872 self-dependent south Brazilians aged over 60 using a questionnaire and oral examination. The subjects perceived chewing as an important aspect of QOL, both physically and psychologically, listing absence of teeth and lack of bite force as physical factors adversely affecting QOL, and difficulty of chewing as a negative psychological factor. Brennan et al.4) analyzed tooth loss and QOL in 879 Australians aged 45 to 54 (response rate of 43.8%) with 3 types of questionnaire and oral examinations by dentists. Chewing ability was regarded as a factor influencing both oral and systemic QOL. Bagewitz et al.3) carried out a questionnaire-based survey on level of interest in oral health in 1974 individuals in Sweden aged 50 to 70 (response rate of 66%) using Oral Health-Related Quality of Life (OHRQOL). They found that these individuals took a greater interest in how many teeth were present than in what type of denture to wear, and that opinion was mixed on the cost of dental care. These studies on people under the age of 80 based mostly on questionnaires and subjective perception of dental status unanimously showed high levels of interest in oral health and QOL.
Devices capable of objectively assessing oral function, particularly occlusal force, have been developed2,9,14). A pressure-sensitive film (Dental Prescale; Fuji Photo Film Co., Tokyo) is one such device10,20) which has been used for occlusal force measurement in a number of studies5,6,8,11,13,15,16,18). It is designed to quantify occlusal pressure from occlusal contact marked on a thin horseshoe-shaped strip of film. This offers a highly advantageous method for assessing bite force in epidemiological surveys, and the data obtained provide good guidelines for the planning of oral health strategies11) for any generation18).
The purpose of this study was to compare number of present teeth and occlusal force between people in their sixties attending a college for the elderly and 8020 achievers in order to clarify the relationship between presence of teeth and oral function. We believe the results will contribute to the design of oral health promotion targeting the elderly, thus increasing the number of 8020 achievers.
Materials and Methods
Forty-six students with an average age of 66.9 years (22 men, 24 women) enrolled at a college for the elderly in Chiba City participated in the study. All were subjected to oral examination and measurement of occlusal force. Occlusal force was measured and evaluated using a pressure-sensitive film and its analyzer (Dental Prescale 50H type R and OCCLUZER FPD-703; Fuji Photo Film Co.). Data obtained from fifty-two 8020 achievers (28 men, 24 women)18) were used for a comparison (Table 1).
With each subject sitting on a chair, head position was adjusted to bring, as much as possible, the Frankfort horizontal plane in parallel with the floor. The subject was asked to bite the pressure-sensitive film for 3 seconds with maximal bite force. The film has a layer of microcapsules containing a color former that reacts with an adjacent colordeveloping layer when crushed upon biting with the entire dental arch. Different densities of color are produced depending on the magnitude of biting force. These are then used to calculate amount of pressure per unit area. These values are added to determine the subject’s total occlusal contact area and occlusal force. Methods for standardized dental examination, analyses and procedures for human subject protection and consent have been previously described12). A multiple regression analysis was performed in order to clarify whether occlusal force depended on number of teeth more than age; occlusal force was considered as an objective variable and age, present teeth and gender as independent variables.
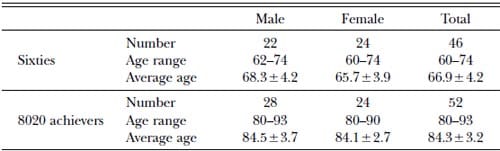
Table 1 – Characteristics of subjects in this study
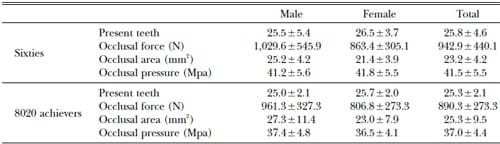
Table 2 – Results of subjects in this study
Results
Average number of present teeth was 25.8 (Table 2). This far exceeded the result obtained in the MHLW dental health survey of individuals in the same age range (15 teeth), and was comparable to the value of 8020 achievers (25.3 teeth)18). Although average number of teeth showed no significant difference between the two groups, three subjects with under 20 teeth were included in the sixties group. Almost half of the present teeth, 40.1% in the sixties group and 44.3% in the eighties group, respectively, were treated; un-treated teeth were very few (under 1%) in both groups.
None of the study subjects had anterior crossbite, the same finding as in 8020 achievers. Classification was as follows: normal occlusion, 37.3%; maxillary protrusion, 32.6%; crowding, 20.0%; deep bite, 8.7%; spaced arch, 2.2%; unknown, 2.2%.
Occlusal force (N) is expressed as occlusal contact area (mm2) multiplied by occlusal pressure (Mpa). Average occlusal force in the study subjects was 942.9±440.1N (1,029.6± 545.9 N for men, 863.4±305.1 N for women) (Table 2). No statistically significant differences in average value (student t -test) of occlusal force, occlusal area or occlusal pressure were noted between the two groups (Table 3). The results of the multiple regression analysis (SPSS, Ver.16) revealed that the standard coefficient of present teeth was 0.366, that of age was -0.023 and that of sex was -0.220 (Table 4).
Discussion
The results of the present study showed no significant difference in occlusal force between the participants, who were in their sixties, and 8020 achievers. Kono8) used Dental Prescale film to measure occlusal force in individuals aged 60 to 87 who were living independently. Measurement included not only natural teeth, but also prostheses replacing missing teeth for restoration of chewing function. Average occlusal force was 502.4± 338.4 N for men and 372.2±262.6 N for women. Among the three age groups studied, the over-80 age group showed significantly lower occlusal force. Average numbers of present teeth for the entire sample were 17.9 for men and 17.3 for women. These results suggest that age, rather than number of present teeth, accounts for lower occlusal force when fewer teeth are present. Miura et al.11) measured bite force in 349 healthy and 24 frail elderly persons aged 65 to 74. Significant differences in bite force at p<0.05 were noted between healthy and frail for both sexes. Average numbers of present teeth and occlusal force measurements were 7 teeth and 408 N for healthy men, 2 teeth and 196.0 N for frail men, 4 teeth and 243.5 N for healthy women and 4.5 teeth and 130 N for frail women.
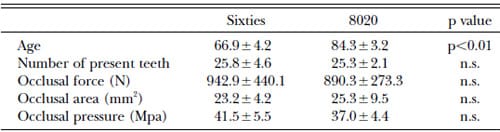
Table 3 – Comparison of age, number of present teeth and Dental Prescale data
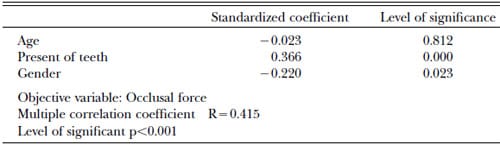
Table 4 – Results of multiple regression analysis
Shinogaya et al.15) measured bite force with Prescale film in young subjects in their twenties (12 Danish women, 12 Japanese men and 12 Japanese women), and 10 senior Japanese men and women in their fifties and sixties. All subjects had 28 teeth. Although a sex difference was observed between young Japanese men and women (1,616.9 N for men, 1,100.7 N for women, p<0.01), no age-related difference was observed (1,616.9 N for young Japanese men, 1,650.8 N for 53–62 age group). In one study comparing occlusal force measured with Prescale film between 8020 achievers and adults in their twenties with normal occlusion, Takeuchi et al.18) found no significant difference between the two groups (979.2 N for young adults, 890.3 N for 8020 achievers). These results suggest that number of present teeth exerts a greater influence on the study results than age.
Ansai et al.1) and Takata et al.17) found that number of foods a subject could chew was related to satisfaction, and that number of sound teeth was related to cognitive function in 60– 65-year-old individuals. They suggested that chewing and number of teeth in the elderly population was related to QOL, ADL, physical fitness, cognitive function and mortality.
The relationship between dental status, in terms of number of teeth present, and diet and nutritional status was analyzed by Nowjack- Raymer et al.12) in a representative sample of US civilian, non-institutionalized adults aged 25 years and older who did not wear dental prostheses to replace missing teeth. The authors attributed frailty to weak occlusal force.
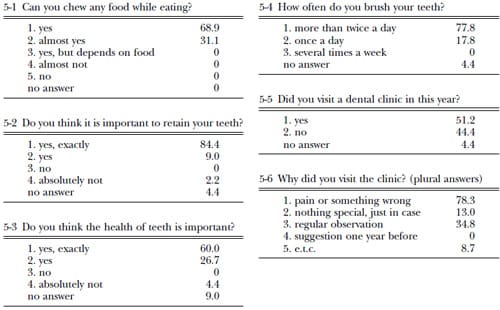
Table 5 – Questionnaire on oral condition and the results (%)
The results of these studies suggest that age is not a determinant of occlusal force in the presence of many teeth, including functional teeth. The subjects of the present study showed a favorable occlusal relationship, another positive factor contributing to higher occlusal force, in addition to many present teeth.
The results of the multiple regression indicates that occlusal force depends on number of present teeth more than age, in other words occlusal force is unaffected by aging if many teeth are present.
Furthermore, these subjects were attending a college for the elderly. They may represent a special group of people, in that they have a high level of intellectual curiosity. Their average number of present teeth was far greater than that found in people of the same age in the MHLW survey (15 teeth). In an earlier study carried out by this group. Yamaguchi et al.21) also reported, a larger number of present teeth (average number of teeth was 26.1; men, 25.9; women, 26.6 teeth) among people attending a college for the elderly. These findings suggest a positive correlation between intellectual curiosity and number of present teeth. However, further study is needed comparing sophisticated and not-not-sophisticated group to clarify this finding.
According to some of the answers given to our questionnaire on daily life, the subjects appear to take care of their oral health (Table 5). If current oral health status is maintained, these subjects are expected to achieve the 8020 goal and maintain adequate occlusal force, allowing them to continue to enjoy food.
References
- Ansai T, Takata Y, Soh Y, Akifusa S, Sogame A, Shimada N, Yoshida A, Hamasaki T, Awano S, Fukuhara M, Takehara T (2007) Relationship between chewing ability and 4-year mortality in a cohort of 80-year-old Japanese people. Oral Dis 13:214–219.
- Atkinson HF, Ralph WJ (1973) Tooth loss and biting force in man. J Dent Res 52:225–228.
- Bagewitz IC, Soderfeldt B, Palmqvist S, Nilner K (2007) Oral prostheses and oral healthrelated quality of life: a survey study of an adult Swedish population. Int J Prosthodont 20: 132–142.
- Brennan DS, Spencer AJ, Roberts-Thomson KF (2008) Tooth loss, chewing ability and quality of life. Qual Life Res 17:227–235.
- Ferrario VF, Sforza C, Serrao G, Dellavia C, Tartaglia GM (2004) Single tooth bite forces in healthy young adults. J Oral Rehabil 31: 18–22.
- Hattori Y, Okukawa H, Watanabe M (1995) Bite force distribution on the dental Arch by using Dental Prescale. J Nippon Hotetsu Shi 38:835–841. (in Japanese)
- Hugo FN, Hilgert JB, de Sousa Mda L, Cury JA (2009) Oral status and its association with general quality of life
in older independentliving south-Brazilians. Community Dent Oral Epidemiol 37:231–240. - Kono R (2009) Relationship between occlusal force and preventive factors for disability among community-dwelling elderly persons. Nippon Ronen Igakkai Zasshi 46:55–62. (in Japanese)
- Laurell L (1985) Occlusal force and chewing ability in dentitions with cross-arch bridges. Swed Dent J Suppl 26:160.
- Matsui Y, Ohno K, Michi K, Suzuki Y, Yamagata A (1996) A computerized method for evaluating balance of occlusal load. J Oral Rehabil 23:50–55.
- Miura H, Watanabe S, Isogai E, Miura K (2001) Comparison of maximum bite force and dentate status between healthy and frail elderly persons. J Oral Rehabil 28:592–595.
- Nowjack-Raymer RE, Sheiham A (2003) Association of edentulism and diet and nutrition in US adults. J Dent Res 82:123–126.
- Ohkura K, Harada K, Morishima S, Enomoto S (2001) Change in bite force and occlusal contact area after orthognathic surgery for correction of mandibular prognathism. Oral Surg Oral Med Oral Pathol 91:141–145.
- Ragalo SC, Santos CM, Vitti M, Regalo CA, de Vasconcelos PB, Mestriner W Jr, Semprini M, Dias FJ, Hallak JE, Siéssere S (2007) Evaluation of molar and incisor bite force in indigenous compared with white population in Brazil. Arch Oral Biol 53:282–286.
- Shinogaya T, Bakke M, Thomsen E, Vilmann A, Sodeyama A, Matsumoto M (2001) Effects of ethnicity, gender and age on clenching force and load distribution. Clin Oral Invest 5: 63–68.
- Sondang P, Kumagai H, Tanaka E, Ozaki H, Nikawa H, Tanne K, Hamada T (2003) Correlation between maximum bite force and craniofacial morphology of young adults in Indonesia. J Oral Rehabil 30:1109–1117.
- Takata Y, Ansai T, Sonoki K, Soh I, Takehara T (2008)Teeth or chewing and QOL. Nippon Rinsho 66:401–410. (in Japanese)
- Takeuchi F, Miyazaki H, Nomura M, Motegi E, Harazaki M, Yatabe K, Yamaguchi H, Hirai M, Sato K (2005) Report on occlusal condition and occlusal force measured with a pressure sensitive film in elderly persons over 80 years old with at least 20 teeth. The Shikwa Gakuho, 105:154–162. (in Japanese)
- Ueno M, Yanagisawa T, Shinada K, Ohara S, Kawaguchi Y (2008) Masticatory ability and functional tooth units in Japanese adults. J Oral Rehabil 35:337–344.
- Watanabe M, Hattori Y, Satoh C (1995) Bite force distribution on the dental arch in normal dentition, Brain and Oral Function, Morimoto T, Matsuya T, Tanaka T eds, p. 399, Elsevier Science, Amsterdam.
- Yamaguchi T, Motegi E, Nomura M, Miyazaki H, Narumiya Y, Takeuchi F, Kaneko Y, Shimizu T, Soejima U, Sasaki M, Ebihara T, Yamaguchi D, Harazaki M, Yamaguchi H, Sekiguchi M (2002) Oral examination and bone mineral density of people in senior college at Tateyama, Chiba. J Japan Acad Occlusion Health 8:27– 30. (in Japanese)
![]()