

Article
Related Links
Estevam Barbosa de LAS CASAS1, André França de ALMEIDA2, Carlos Alberto CIMINI JUNIOR3, Paulo de Tarso Vida GOMES4,
Tulimar Pereira Machado CORNACCHIA5, Jorge Milton Elian SAFFAR6
- Ph.D, M.Sc. Professor, Department of Structural Engineering, Federal University of Minas Gerais, Belo Horizonte, MG, Brazil.
- Researcher, Department of Mechanical Engineering, Federal University of Minas Gerais, Belo Horizonte, MG, Brazil.
- Ph.D, M.Sc. Professor, Department of Structural Engineering, Federal University of Minas Gerais, Belo Horizonte, MG, Brazil.
- Ph.D, M.Sc. Researcher, Center for Development of Nuclear Technology (CDTN), Belo Horizonte, MG, Brazil.
- Ph.D, M.Sc. Professor, Department of Restorative Dentistry, Federal University of Minas Gerais, Belo Horizonte, MG, Brazil.
- Researcher, Technological Center Foundation of the State of Minas Gerais (CETEC), Belo Horizonte, MG, Brazil.
Abstract
Oral forces applied to human teeth during biting and mastication are normally described in the literature only in terms of their axial components. The purpose of this study was to fully determine the spatial characteristics of the oral resultant force – its normal and tangential components – for a given individual. A load cell was especially manufactured to measure oral force and was temporarily implanted as a prosthetic device in the dental arch of a volunteer, replacing his missing upper first molar. The mastication and occlusion tests were carried out in such a way the cell should withstand the loads applied to the molar, and its state of strain was recorded by strain gauges attached to it. Based on the results of these tests and using balance equations, normal and tangential components of the resultant oral force were determined. For direct occlusion, without interposition any obstacle between cusps, a peak normal force of 135 N was recorded simultaneously to a tangential force of 44 N. For mastication of biscuits, a peak normal force of 133 N and a tangential force of 39 N were obtained.
Uniterms: Dental occlusion; Dental prosthesis; Bite force.
Introduction
The values of forces acting on teeth have been extensively addressed in the literature1-11. These values are usually obtained when a tooth is under loading due to either mastication or biting. Biting is understood as the act of breaking food in large pieces that will be further chewed. In this process, a tooth is subjected to what is called occlusal loads. In mastication, the forces are briefer and less intense.
Cimini, et al.4 (2000) published a literature review addressing the different methods of measuring oral forces. Howell and Manly7 (1948) used an inductance strain gauge to record the maximum occlusal load in a group of men aged 20 to 30 years. The measurements were repeated for days and the occlusal loading values in the molar region ranged from 391 to 881 N.
Waltimo and Konomem11 (1993) measured the maximum occlusal force, which occurs in the molar region when the mandible is almost in the intercuspal position and the vertical jaw opening is between 9 and 20 mm. A load cell, built to comply with these factors, had a quartz force transducer and should be bitten by the patients. Its length was such that the recorded values were actually the force withstood by more than one tooth. A maximum force of 722 N was recorded. Duyck, et al.5 (2000) measured the oral forces developed in oral implants. Extensometers were attached to the implant abutments and volunteers were asked to bite as hard as they could, allowing the strain acting in the abutments to be measured. These values were used to calculate the occlusal forces and bending moments, which reached peaks of 170 N and 70 N.cm, respectively. These results are, in fact, part of the total mandible force acting on each abutment and should not be compared to the occlusal force normally withstand by one tooth.
The measuring methods usually reported for masticatory forces are different from those used for occlusal forces. Anderson1-3 published three articles aimed at measuring forces that act on teeth during mastication. In the first article1, a small strain gauge was placed on the crown of a mandibular first molar of a patient who was asked to chew bilaterally four pieces of biscuit at 11-second intervals. The maximum mastication force ranged from 39 and 59 N. In a second article, Anderson2 (1956) used a strain gauge extensometer to measure masticatory forces and also maximum pressure during contact for mastication of biscuit, carrot and raw meat. In this calculation, this author considered pressure distribution to be uniform over tooth surface. Four patients were asked to chew bilaterally and the results ranged from 59 N to 69 N for maximum masticatory load. In his third article, Anderson3 (1956) used the same measuring methods, but with the goal of evaluating the maximum masticatory force for the entire molar surface. The obtained results varied between 112 and 146 N for biscuit, 118 and 134 N for carrot and 71 and 114 N for raw meat.
In a study about masticatory forces, Howell and Brudevold8 (1950) used the same measuring principle as that of a previous article7. However, this time the extensometer was inserted under an artificial tooth placed in a set of dentures of a 48-year-old patient that had been wearing complete dentures for five years. The sensors were placed in the position of a first molar, first premolar and second premolar and were tested during mastication of shredded coconut, peanuts and raisins. For the first molar, maximum masticatory forces of 39, 44 and 64 N were recorded for peanut, shredded coconut and raisins, respectively. Gibbs, et al.6 (1981) used an extraoral method based on sound transmission for measuring masticatory loads. Twenty volunteers participated in mastication assays with cheese, raw carrots, beef, raisins, bread, chewing gum and peanuts. The average maximum masticatory force was of 261 N. Neill, et al.10 (1989) used a method in which EMG (electromyography) sensors recorded electrical activity of masseter muscles in 10 volunteers. The results indicated an average maximum masticatory force of 675 N for beef, 673 N for carrot, 788 for nut, 700 N for biscuit and 550 N for gum.
A summary of results found in specialized literature for occlusal and masticatory forces on molars is shown on Table 1. If these values are to be used as reference for a load measuring test in teeth, the adopted methodology must be taken into account because it can considerably alter the results. Therefore, Table 1 indicates: (i) whether the method allowed measurement of forces applied by a single tooth (as opposed to a group of teeth); (ii) w
hether the occlusal contact was direct; and, if not, (iii) what was interposed between antagonist molars.
Considering this brief review of literature regarding measurements of oral forces in teeth, it is inferred that despite the large number of studies addressing this subject, the results vary greatly, primarily due to differences in measurement methods, but also due to the inherent variability of the biting process. Moreover, the results are mostly given in terms of the normal force component acting on the tooth, whereas the tangential component is seldom mentioned, which does not allow calculation of the actual resultant force (including its module and direction) acting in a tooth. Duyck, et al.5 (2000) determined the bending moment, which would allow calculation of a tangential force (dividing it by the lever arm) that corresponds to a situation without any normal component in the force vector. As far as it could be ascertained, there is no study describing tooth loading from a resultant force with normal and tangential components.
The goal of this study was to determine the module and direction of the resultant force acting on a first molar using a force transducer especially designed and fabricated for this purpose. Non-axial load components are known to produce high stresses on tooth structure9, occasionally leading to enamel fracture and to the development of clinical pathologies, such as abfraction. A mechanical analysis of such cases has as a basic requirement the knowledge of realistic loading conditions to be applied to the model, representing the actual situation during biting, mastication and eventually parafunction. A more precise knowledge of the forces acting on teeth might also represent improvements for dental implants, restorative techniques and orthodontic appliances.
Material and Methods
The custom-made load cell was a square section column type device designed to measure the force withstood by a single tooth and provide sufficient data to calculate the resultant force in all its characteristics. The load cell was implanted in a spot in the upper dental arch of patient with a flawed dentition and therefore acted as a dental implant, carrying out the functions of the missing tooth. Deformations were measured by four strain gauges placed on each face of the load cell’s main column, which should resist the loads. The results were used as a basis to determine the exerted forces.
This load cell was composed of three parts: (i) the base, which attached the implant to the dental arch; (ii) the main column; and (iii) the supporting disc for dental crown mold. The base of the load cell was a mold of the root of the missing tooth (upper irst molar) where the cell was implanted. This part was attached to the bottom of the main column. The main column had a square cross-sectional area, with its side measuring 3 mm, and a 2 mm diameter concentric hole. Its height was 4 mm and the four extensometers were glued to its faces. These sensors were located in the longitudinal central line and at a distance of 2.2 mm from the top of the column. A disc (8 mm in diameter; 0.8-mm thick) was placed on top of the column to support the crown’s ceramic mold that replicated the intercuspal contact. The cell body was fabricated in nickel-chromium alloy with modulus of elasticity E = 197500 MPa. Figure 1 shows two pictures of the load cell: one in detail, but without the crown mold, and the other with the crown mold, after implantation.
A pressure pre-sensor was used simultaneously to the load cell, with the purpose of comparing the results yielded by the two measuring devices (Pressurex–Tactile Pressure Indicating Film; type: medium; SPI, Sensor Products Incorporated, 300 Madison Avenue, Madison, NJ USA). After being subjected to the occlusal pressure, the films displayed red spots of different intensities and were sent to the manufacturer to be digitalized so that the resultant force applied over the film could be determined.
The research project was submitted to the Ethics in Research Committee of the Federal University of Minas Gerais and approved under number ETIC 06/02. The chosen volunteer fulfilled the study requirements of having tooth height greater than average (so that the cell would not obstruct normal occlusion) and having a missing maxillary first molar where the cell could be implanted. The experiment lasted about 30 minutes; within this period, the force transducer was cemented in the patient’s tooth root, the measurements were made and the implant was removed. The following tests were made: three occlusions without any object between the antagonist teeth, four occlusions with the pressure pre-sensor between the teeth, mastication of carrot and biscuit and two measurements of the patient’s emulating bruxism. Figure 1 shows the implanted cell during the experiment.
The measurements recorded by the load cell indicated the strain at each one of the four extensometers for every instant in time. The strain ε in that point of the column relates to the stress σ by Hooke’s Law: σ = Ε • ε
The deformation of the load cell was considered to be caused entirely by the resultant force acting on the geometric center of the supporting disc (which coincides with the main column’s axis). This force has both tangential and normal components.
The deformation of the load cell was considered to be caused entirely by the resultant force acting on the geometric center of the supporting disc (which coincides with the main column’s axis). This force has both tangential and normal components.
The normal component has the same effect on all the four strain gauges, being responsible for compressing them to a level of uniform deformation (en). This strain can be associated to stress by Hooke’s Law, which relates to the normal component of the resultant force (Fn) by the following equation:
![]()
where A is the cross-sectional area of the column.
The tangential component of the resultant force acts in the occlusal plane and has a different effect on each side wall of the column. The extensometers were numbered 1 to 4, 1 being the strain gauge located closest to the buccal wall, 2 at the distal wall, 3 at the lingual wall and 4 at the mesial wall. The tangential force can be further decomposed in components in the 1-3 axis direction and 2-4 axis direction. These components cause a bending moment due to the 2.2 mm lever arm, which leads to strain throughout the column. Bending moments cause normal strain that add to the uniform strain induced by the normal component of the resultant force. The moment caused by component 1-3 of the tangential force does not have an effect in faces 2 and 4 of the column, and vice-versa. Normal deformation due to bending moments was calculated using the following equation:
![]()
whereM is the moment given by the product of the force (component 1-3 or 2-4 of the tangential force) by the lever arm; l is the side of the square cross-sectional area; I is the moment of inertia of the cross-sectional area and E is the modulus of elasticity.
The moment causes tension on one face of the column and compression on the opposite face. Shear force effects were not considered because the extensometers are in the outer surface of the column, where this stress component is null.
From the above-mentioned considerations, the strain measured by each strain gauge can be reduced to the following equations:
The strain due to the normal component of the resultant force (εn</sub >) was determined by the average of the deformation measured by the four extensometers, which is consistent with Equations 4 to 7. This result leads to the normal component of the resultant force, using Equations 1 and 2. The difference between Equations 4 and 6, and Equations 5 and 7 provided the values of εM(1-3) and εM(2-4), respectively. The values for both bending moments were obtained with the results of Equation 3. This relates to the components 1- 3 and 2-4 of the tangential force by the following equation: M = F.aL; (Equation 8) where aL is the lever arm. The module of both forces 1-3 and 2-4 is the tangential component of the resultant force.
Alternatively, the forces acting on a tooth can be represented by a single normal force acting on the surface pressure center, which does not need to be coincident with the geometric center. The pressure center is obtained by real pressure distribution throughout that surface. The results of pressure film showed such a distribution (Figure 2). However, it was noted that the process of pressure recording in the film is cumulative and the results represent pointwise peaks during biting rather than pressures at a given time. As a result, an instantaneous pressure center cannot be obtained from the film results. This is further discussed in the Results section.
Results
For each measurement, the resultant force, its normal and tangential components, the vertical inclination angle of the resultant force and the angle of the tangential component in the occlusal plane were calculated. All these parameters were monitored as to how they fluctuate in time during occlusion or mastication.
Initially, it is interesting to present the results for the instant of maximum resultant force, as these values can be compared to the results of previous studies. It should be mentioned that the normal component is responsible for most part of the resultant force. Therefore, the peak resultant force occurred simultaneously to the peak normal component force. Table 2 presents, for each measurement, the results for the maximum resultant force, the normal and tangential components, and the force measured by the presensor film (when it was used). The angle ? is determined between the resultant force and the direction normal to the occlusal plane while the angle φ is the direction of the tangential component in the occlusal plane, and refers to the axis joining the buccal and lingual faces, starting at the lingual end and measured in the counterclockwise direction (Figure 1).
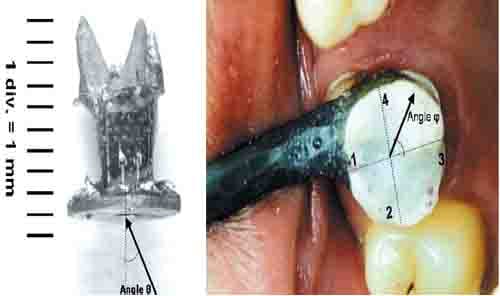
FIGURE 1- Left: Detail of load cell without the crown’s mold and angle of vertical inclination θ. Right: Load cell implanted in the patient and angle φ of the tangential component in the occlusal plane
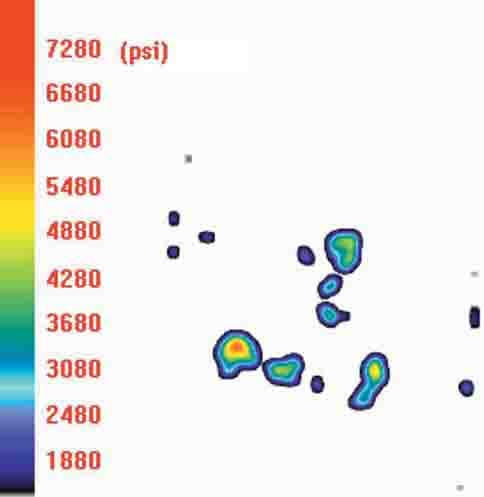
FIGURE 2- Pressure distribution in the premolar occlusal plane
Another aspect of oral forces recorded in this experiment was the evolution in time of such forces along the duration of occlusion. This analysis was limited to measurements of direct occlusal contact, which presented more uniform results. Figure 3 shows the evolution of the tangential and normal forces along time for occlusion tests without films 1, 2 and 3. In these figures, a negative sign has physical meaning only for the normal component (indicating compressive forces) because in case of tangential forces their direction will be determined by angles φ and θ.
Discussion
The first observation comes from the comparison of the results of the present study (Table 2) to those of previous studies (Table 1). The values obtained in this study were significantly lower, which is not necessarily inconsistent, as mentioned before. The different measuring methods yielded great amplitude for the occlusal force values and did not allow the establishment of any standard value for occlusal forces in molars. It was expected that the results of this experiment would be smaller than those obtained other authors9,10, who measured the total force exerted by more than one tooth. Most articles addressing occlusal forces describe experiments in which the occlusal contact was indirect. In the present study, the tests were held with direct and indirect occlusal contact. Our results show that indirect occlusal contact acts increasing the occlusal force. This is also observed in the results of other authors (Table 1).
In the present experiment, it was possible to compare the results of force measurements made by the load cell and by the sensor film. Four occlusion tests were held with forces being recorded by both measuring devices. As shown on Table 2, it was not possible to establish a connection between the force measured by the sensor film and any component of the resultant force measured by the load cell. Certain aspects of the pre-sensor film technique that could lead to imprecise measurements were then reviewed. Firstly, is the fact that, from the analysis of the stained film, a maximum force is obtained acting over the area of the film as if an occlusion were an instantaneous event. During the assay, it was noted that an occlusion lasted up to 15 sec and, during this time, the subject was unable to sustain the same force pattern. Supposing that the subject initially pressed harder towards the mesial tooth surface and then towards the distal tooth surface, the film would then register peak forces that are in fact a result of the combination of both effects, but that do not occur simultaneously in time. Secondly, a relevant aspect affecting the film measurements is that the sensor records forces acting normal to its surface, which do not stay unaltered – the film deforms and takes the form of the crown. Therefore, it is impossible to determine the direction of the force that acted on the film surface. From these assessments, it is possible to conclude that the pre-sensor film is not a precise instrument for measuring oral forces.
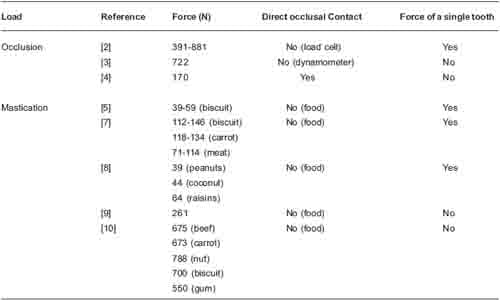
TABLE 1- Occlusion and mastication loads for the first molar
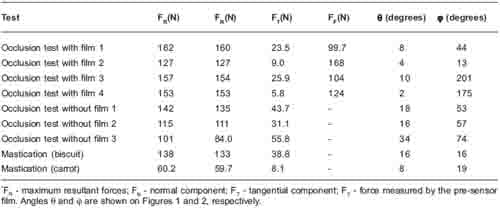
TABLE 2- Results of maximum resultant force*
Table 2 shows the values of the tangential component of the maximum resultant forces. Its values ranged from 5.8 N to 55.8 N. From the seven measurements of occlusal forces, only in two cases the tangential component represented less than 10% of the maximum resultant force. The tangential force can cause a deviation of almost 35º towards the resultant force (away from the normal direction to tooth surface). Additionally, as indicated by the obtained results, it appears that the presence of a device between the antagonist teeth (such as the pre-sensor film) acts attenuating this effect. It is clear that a value of maximum normal occlusal force is a poor description of a tooth loading status and that the effects of the tangential force should not be dismissed without proper examination.
The results for maximum mastication load were consistent with the values reported in previous studies (Table 1). During mastication, a tooth is subjected to forces exerted by other teeth, tongue or food. The combination of these effects was measured by the load cell and cannot be easily separated.
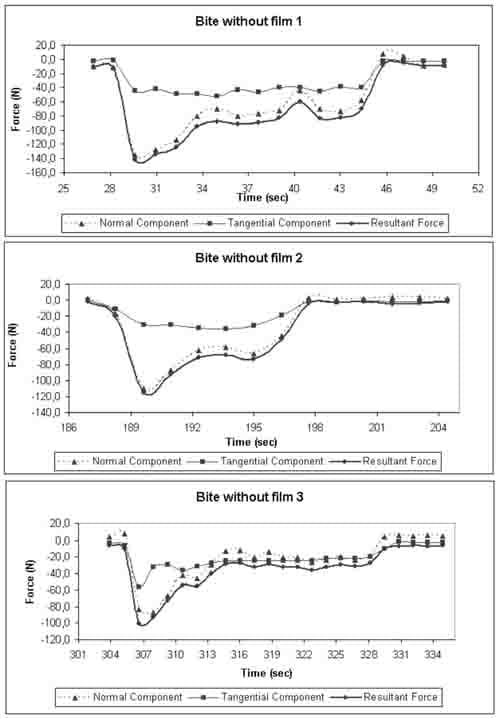
FIGURE 3- Results for occlusion assays without film
Three main considerations can be made from analys
is of Figure 3. Firstly, the subject, when tested for direct occlusal loads, initially exerted the highest value for the resultant force and was unable to sustain that magnitude of forces throughout the duration of the effort. In the measurements with the sensor film between the molars, the force magnitude varied differently in time for each measurement without a recognizable pattern. Secondly, the tangential components of the forces assumed an almost constant value during the entire occlusion period. It is noteworthy that the direction of these forces varied, but its modulus remained almost unaltered (between 30 N and 40 N) – a significant value, considering peak resultant forces between 100 N and 140 N. Thirdly, even during biting, the forces did not remain constant in time. The modulus and direction changed during the contact of the occlusal surfaces, and the consideration of a static loading should take this fact into account. In the present case, as tangential forces were relatively constant, peak stresses would occur for the highest resultant forces, as the force variation in time affects mostly its axial component. Mastication is expected to have an even more pronounced dynamic character in loading.
The direction of the resultant force can be represented by the values of the normal and tangential components and the direction of the latter in the occlusal plane, measured by the angle φ. Initially, as the resultant force increased rapidly, the tangential forces acted in a direction between the buccal and mesial surfaces, but very close to the normal direction to the buccal surface. This means that the tooth is being pulled towards the vestibule. As the resultant force reaches its peak, the tangential components shifts towards a direction between the mesial and lingual faces (approximately 60º from the normal direction to the lingual plane), the tooth being pulled towards the mouth opening. The tangential force remains in this direction until occlusion is over. Again, this was verified in all measurements of direct occlusal contact. The vertical inclination of the resultant forces can be obtained from the combination of the normal and tangential components shown in Figure 1. Initially, when the tangential component is nearly zero, the angle measured approximately 10º. The tangential and normal components increased until the resultant force reached its maximum, at which moment the vertical angle was 16º. Thereafter, the normal component decreased while the tangential component remained almost constant, resulting in an angle of approximately 30º. This pattern was not the same for the different measurements.
Conclusions
A special load cell was manufactured and implanted in a patient with flawed dentition. The measurements allowed determining the direction and modulus of the resulting oral force that acted on the implant, demonstrating the effectiveness of the proposed device and methodology. It is clear that the obtained results cannot be generalized as a case of normal occlusion. The particularities of the subject’s dentition and measuring method show that the acts of biting and chewing are more complex than the existing standards of oral forces in an assumed normal occlusion. The relevance of the tangential component of the occlusal force in the obtained results indicates that it should be accounted in the mechanical analysis of dental problems. The results of the present study show that simplifying the occlusal force as acting normal to the occlusal surface can lead to erroneous mechanical interpretation of essential phenomena in the oral environment and that further investigation of its tangential component is needed. Another important outcome is the transient character of the forces, which vary in modulus and direction with time.
References
- Anderson DJ. A method of recording masticatory loads. J Dent Res. 1953;32:785-9.
- Anderson DJ. Measurement of stress in mastication. I.J Dent Res. 1956;35:664-70.
- Anderson DJ. Measurement of stress in mastication. II. J Dent Res. 1956;35:671-3.
- Cimini CA Jr, Gouvêa PHP, Las Casas EB, Cornacchia TPM. Loads in teeth: a critical review. In: Proceedings of the METMBS’2000: The 2000 International Conference on Mathematics and Engineering Techniques in Medicine and Biological Sciences; 2000; Las Vegas, NV. CSREA Press, 2000. v. 2, p. 649-55.
- Duyck J, Van Oosterwyck H, De Cooman M, Puers R, Vander Sloten J, Naert I. Three-dimensional force measurements on oral implants: a methodological study. J Oral Rehabil. 2000;27:744-53.
- Gibbs CH, Mahan PE, Lundeen HC, Brehnan K, Walsh EK, Holbrook,WB. Occlusal forces during chewing and swallowing as measured by sound transmission. J Prosthet Dent. 1981;46:443-9.
- Howell AH, Manly RS. An electronic strain gauge for measuring oral forces. J Dent Res. 1948;27:705-12.
- Howell AH, Brudevold F. Vertical forces used during chewing of food. J Dent Res. 1950;29:133-6.
- Las Casas EB, Cornacchia TPM, Gouvêa PH, Cimini CA Jr. Abfraction and anisotropy: effects of prism orientation on stress distribution. Comput Methods Biomech Biomed Engin. 2003;6:65-76.
- Neill DJ, Kydd WL, Nairn RI, Wilson J. Functional loading of the dentition during mastication. J Prosthet Dent. 1989;62:218-28.
- Waltimo A, Kononen M. A novel bite force recorder and maximal isometric bite force values for healthy-young adults. Scand J Dent Res. 1993;101:171-5.
![]()