

Article
Related Links
Antun Salamon1, Tomislav Salamon2, Vasilije Nikolic3, Radivoje Radic3, Tatjana Nikolic4 and Ana Jo-Osvatic2
1 Department of Surgery, University Hospital »Dubrava«, Zagreb, Croatia
2 Department of Anatomy, School of Medicine, University of Zagreb, Zagreb, Croatia
3 Department of Anatomy, School of Medicine, University »J. J. Strossmayer«, Osijek, Croatia
4 Department of Physical Therapy and Rehabilitation Medicine, University Hospital of Traumatology, Zagreb, Croatia
Abstract
Talocrural joint injuries are among the most common injuries of the joints and therefore there is a need for a holistic approach to analysis of morphology, biomechanics and visualization of the talocrural joint ligamentary apparatus in different positions. The research was carried out on 20 fresh and conserved anatomical specimens of the lower leg on which X-ray, computed tomography, ultrasonography and stress analysis were performed before and after the lesion of ligaments. Also the gait of 130 adults without (100) and with ligament and joint capsule lesion (30) was analyzed by infrared telemetry. After complete discission of the lateral ligaments, arthrography and CT could register the lesion, while X-ray and ultrasonography could not detect it. Gait analysis of healthy and injured leg showed that the injured leg was significantly less loaded.
Keywords: talocrural (ankle) joint, ligaments, injury
Introduction
Talocrural joint injuries are among the most common injuries of the joints. Statistical analyses of many authors reveal that approximately 10% of all injuries comprise capsular and ligamentar injuries, and about 40% of these injuries affect the talocrural joint. Increasing number of authors1 report on diagnosis and therapy of isolated capsular and ligamentar injuries of the talocrural joint, emphasizing the fact that many physicians, and even specialists in traumatology, consider these injuries trivial, and conduct only symptomatic therapy with physical procedures, or do not immobilize the joint long enough2. The consequence of such treatment is often loose, instable ankle, often with recurrent distortions and late posttraumatic arthrosis3,4. These apparently trivial injuries may thus cause certain invalidity if treated improperly, especially in professions where ankles are particularly under stress, as with field workers, athletes and ballet dancers. The treatment of isolated ligamentar ruptures with immobilization for 6 to 10 weeks as recommended by Böhler et al. back in 1976 does not always result in complete ankle stability. The thorn ligament and the capsule of the joint do not always heal in anatomical position, usually because of interposition of either fat, capsular or synovial tissues.
It is evident that there is a need for holistic approach to analysis of morphology, biomechanics5,6 and visualization of the talocrural joint ligamentary apparatus7 in different positions. Using several methods simultaneously in the treatment of this diagnostically and therapeutically problematic ligamentar injury of the talocrural joint will thus establish a minimum of diagnostic procedures in suspected injuries of the ankle ligamentar apparatus. Anatomical specimen is the best model for such kind of investigation. The same specimen could be X-rayed many times without overdoses risk and than could be dissected.
Materials and Methods
The research was carried out on 20 fresh anatomical specimens of the lower leg with all tissues preserved. In all specimens lateral capsular ligamentar injury was simulated by transcutaneous discission. In the first phase the anterior talofibular ligaments were injured, first partially and then completely7. In the next phases, the posterior talofibular ligament and finally the calcaneofibular ligament were transected.

Fig. 1. Ultrasound image of of the lateral ligaments incision with a scalpel.
All specimens, intact and in all phases of lesion, were examined with several radiographic and ultrasonographic methods. X-rays of these samples were made in antero- posterior and latero-lateral, as well as in oblique projections, and also in positions that simulated different ankle movements (Table 1). Focus-film distance was 80 cm. Ultrasonography was made also in different projections with linear probe 7.5 MHz (Figure 1). All specimens were also investigated by serial CT (Figure 2). Several intact specimens were injected by water-soluble contrast Rompacon into the joint cavity8 and then first X-rayed in antero-posterior and latero -lateral projection (Figure 3) and by CT (Figure 4).

TABLE 1 – NUMBER OF INVESTIGATED SPECIMENS BY SPECIFIC METHOD
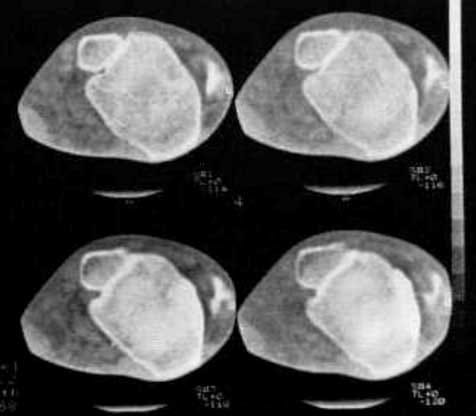
Fig. 2. CT (detail) of the talocrural joint.

Fig. 3. Artrography after artificiallesion of the ligaments (leaking of the Rompacon contrast media from the joint capsula).
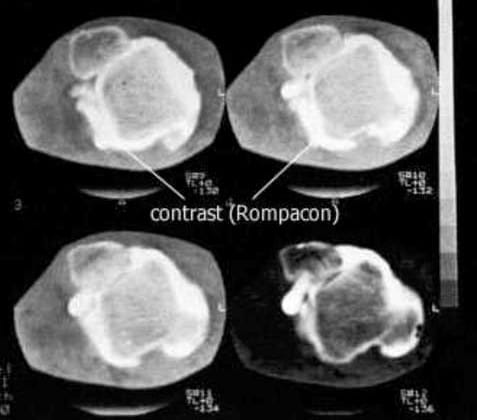
Fig 4. CT arthrography after the lesion of all the ligaments of the lateral group.
After successive lesions, from partial to total, the degree of subluxation and the angle of the talus position were measured by analyzing mobility, first of the intact, and than of the injured specimens in each phase of the lesion. It was assessed in two ways: by measuring on stressed X-rays the distance between the overlapping point of the fibular malleolus and the tibia, and the upper lateral border of the talus, or by measuring the angle between the line passing through the two uppermost points on the articular surfaces of the tibia and the talus (Figure 5).
Contact pressure measurements were performed by placing pressure-sensitive foils (Fuji film Prescale). We used foils of two sensitivities: low and super low. The specimen was placed under stress in the positions of plantar and dorsal flexion, eversion and inversion and loaded statically. Loading (200N and 400N) was transmitted axially through the tiba and the fibula. In each position new foil was placed between articular plates. Areas under greatest pressure were shown in most intense color and the in tensity can be determined in Pascals by specially designed densitometers.
Results
Experiments were performed on 20 anatomical specimens. Only arthrography and CT can detect lesion of the anterior talofibular ligament, while X-ray and ultrasonography (US) could not adequately detect it. Leaking of water-soluble contrast Rompacon from the joint cavity in periarticular tissue on lateral side is the most evident proof of lesion. After complete discission of lateral capsular ligamentar apparatus, lesions were registered also by ultrasonography and by stress X-rays. On anatomical specimens with injected contrast by ultrasonography is diagnosed as intraarticular liquid. Edema or tenosinovitis could not be recognized on our anatomical specimens.
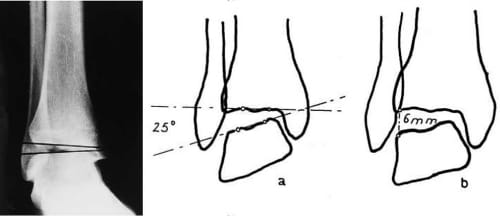
Fig. 5. X-ray (A-P) with marked tibiotalar angle after the lesion of lateral ligaments.
The tibiotalar angles were increased proportionally with stage of ligament lesion (Table 2). In the first group, where only anterior talofibular ligament was discissed, the tibiotalar angle was 8–10 degrees (in comparison with less than 5° in intact specimens). In the joints with lesion of anterior talofibular and calcaneofibular ligaments the tibiotalar angle was 10–15 degrees and in the third group, where all three lateral ligaments were discissed, the tibiotalar angle was between 30 and 45 degrees.
Measurements of contact pressure with pressure-sensitive foils give us a good image of the articular cartilage stress distribution. Figure 6 shows the intraarticular stress distribution in talocrural joint, determined by pressure-sensitive foil on intact (A) and injured specimens after discission of the lateral ligament groups (B). The mean stress on the articular cartilage of the intact joints, loaded with 200 N, was 260 kPa and maximal stress was up to 600 kPa, while with loading force with 400 N mean stress was 540 kPa and maximal stress was 1,270 kPa. In injured joints a concentration of greatest pressures was in anterior and medial parts of the joint up to 1470 kPa, with loading force of 200 N and up to 3,210 kPa with loading force of 400 N (Table 3). The results of the measurement of pressure distribution in tibiotalar joint show that the lesion of the lateral group of ligaments causes the concentration of greatest stress in the medial and posterior parts of the trochlea tali, which will inevitably lead to the damage of articular cartilage and later arthrotic changes, if not treated properly.
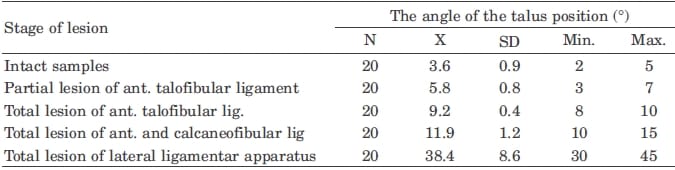
TABLE 2 – THE TIBIOTALAR ANGLE IN INTACT SPECIMENS AND AFTER DISCISSION OF THE LIGAMENTAR APPARATUS
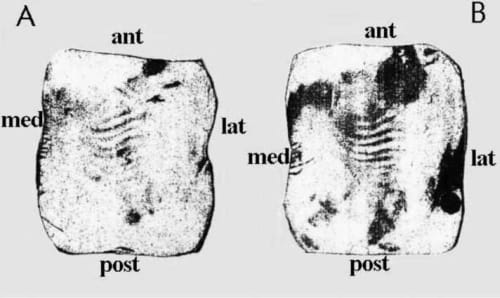
Fig. 6. The distribution of intraarticular pressure load on intact (A) and injured (B) specimens of the talar trochlea (greater color intensity = greater pressure load).
Discussion
Arthrography and CT images of the injured talocrural joint showed that these methods could be used only to diagnose larger ligamentar lesions. Measurements of the distance between the point where the contours of tibia and fibular malleolus overlap and the most prominent part of the lateral border of the talus were not taken into consideration because the possibility for error was too great. The measurement of the tibiotalar angle11 in stressed X-rays is a more accepted method of diagnosing the lesion of the lateral group of ligaments, and this was the method we employed in measuring the size of lesion of the lateral group of ligaments in the talocrural joint.
Articular cartilage will function normally on intermittent loads, with pressures within given optimal range. Articular cartilage is a highly elastic and porous structure so the range of optimal pressure depends on its composition, structure and thickness. The size, shape and position of the contact surface and the pressure change in different movements and positions of the joint, depending on the shape of articular bodies and resulting force.
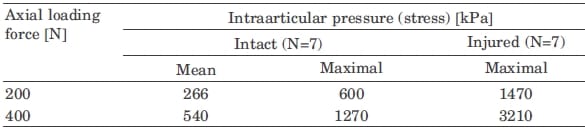
TABLE 3 – INTRAARTICULAR PRESSURE IN INTACT AND INJURED (AFTER TOTAL LIGAMENTAR DISCISSION) TALUCRURAL JOINT MEASURED BY PRESSO-SENSITIVE FOILS (FUJI)
Pressure is not equally distributed over the contact surface of the joint; there are areas of different intensities and areas of maximal pressures. But these areas also change their position depending on the position of articular bodies and possible non-homogeneity of the articular cartilage and subhondral bone. Biomechanical processes in the joint are very complex, which justifies the attempts and need for most exact determination of pressure distribution between articular surfaces in different phases of movement, as we proved in part by this investigation. Our results of the measurement of pressure distribution in tibiotalar joint show that in the lesion of the lateral group of ligaments the concentration of greatest pressures is in the medial and posterior parts of trochlea tali, which will inevitably lead to the damage of articular cartilage and later arthrotic changes if not treated properly, as confirmed by [anti} et al.6 The shape and configuration of articular bodies determine the size of contact surface that transmits the pressure from one articular body to another within the ankle. If unhealed distortions or insufficiencies of the ligamentar apparatus result in inadequate contact between articular surfaces (greater pressure on smaller area), arthrotic changes and later invalidity will result.
For the purpose of preventing arthrotic changes based on the detailed analysis of inadequate pressure distribution many authors8,12,13 have tried to design the method of measuring the pressure on different parts of articular surfaces and so predict the occurrence of arthrosis. That enables the correction of the treatment methods for such lesions, which have been explored by biomechanical system for telemetry according to Santic6,9.
Rehabilitation objectives are restoring the full ranges of motion of ankle joint in all planes, improving the strength of muscles affected by the injury or immobilization and restoring the gait to its pre -injury level14. During rehabilitation treatment we must consider age (poor healing of skin and bone, osteopenia), systemic disease (diabetes, metabolic bone disease), articular involvement (posttraumatic arthritis) and foot compartment syndrome. In addition to various exercises proprioception training must be instituted for all patients. Other physical therapeutic treatment modalities could be also used such as cold, magnetotherapy, ultrasound, electrotherapy and electrical stimulation as a part of strengthening program, as well as medication if necessary.
Conclusion
After analyzing the possibilities of diagnosing ligamentar rupture of the talocrural joint and its instability, and assessing the value of different diagnostic procedures we conclude:
- Smaller lesions of the ligaments of the talocrural joint can be mistaken for milder distorsion and therefore mistreated.
- X-ray, CT as well as arthrography can diagnose only large injuries of the lateral ligaments.
- Tibiotalar angle measuring gives a good insight into the joint lesion, because the greater tibiotalar angle implies the lesion of the lateral group of ligaments and justifies operative exploration.
- Every positively diagnosed lesion of the ligaments of th
e talocrural joint should be treated operatively to reconstruct the joint capsule (capsuloplasty) and thorn ligaments. - Experiments with pressure-sensitive foils proved that an inadequately treated lesion of the talocrural joint leads to uneven and non-proportional load on the articular cartilage, which can result in arthrosis and permanent invalidity of patients.
Acknowledgements
This work was supported by the Croatian Ministry of Science and Technology (grant 0219011).
References
- LIU, S. H., K. E. JACOBSON, J. Bone Jt. Surg. (Br), 77 (1995) 55.
- WATSON-JONES, R.: Fractures and joint injuries. (Livingstone LTD., Edinburg -London, 1976).
- XENOS, J. S., W. J. HOPKINSON, M. E. MULLIGAN, E. J. OLSON, N. A. POPOVI], J. Bone Jt. Surg., 77 (1995) 847.
- WEBER, B. G., W. HUPFUER, Arch. Orthop. Unfall-Chir., 65 (1969) 251.
- NIKOLI], V., M. HUDEC: Principi i elementi biomehanike. ([kolska knjiga, Zagreb, 1998).
- [ANTI], A., V. BILAS, I. LACKOVI], Period. Biol., 104 (2002) 305.
- [ALAMON, A.: Clinical, anatomical and biomechanical characteristics of the capsular and ligamentar injury of the upper ankle joint. In Croat. Ph.D. Thesis. (School of Medicine, University of Zagreb, Zagreb, 1998).
- CASS, J. R., B. F. MORREY, Y. KATOH, E. Y. S. CHAO, Clin. Orthop.,
198 (1985) 110. - ANDRI], V., M. BIELEN, V. NIKOLI], A. JO-OSVATI], A. [ALAMON, Period. Biol., 104 (2002) 311.
- [ALAMON, A., V. NIKOLI], A. JO-OSVATI], V. ANDRI], Period. Biol., 104 (2002) 317.
- ZWIPP, H., S. RAMMELT, R. GRASS, Clin. Pediatr. Med. Surg., 19 (2002) 195.
- BONNIN, J. G., J. Bone Jt. Surg., 47 (1965) 609. 6 (1978) 305.
- HOPPEMFELD, S., V. L. MURTHY: Treatment and rehabilitaion of fractures. (Lippincott, Williams and Williams, Philadelphia, 2000).
![]()