

Article
Related Links
Akitoshi Machida, Kazuomi Sugamoto, Takashi Miyamoto, Hiroaki Inui, Tetsu Watanabe and Hideki Yoshikawa
Department of Orthopaedic Surgery, Osaka University School of Medicine
Abstract
In order to determine whether adhesion of the subacromial bursa leads to impingement, we measured the subacromial contact pressures before and after release of adhesion of this bursa. 18 shoulders with cuff tears and adhesion of the subacromial bursa were evaluated in 8 male and 10 female patients, of mean age 62 (53–71) years and who had no particular limitation of shoulder motion. We recorded subacromial pressures using a very sensitive film inserted under the acromion during surgery. In passive scapular plane elevation (scaption) at 100°, the mean subacromial contact pressure and area declined from 1.43 (SD 0.23) MPa before release to 1.14 (SD 0.35) MPa after release (p < 0.001), and from 163 (SD 81) mm2 before release to 80 (SD 46) mm2 after release (p < 0.001), respectively. We suggest that adhesion of the subacromial bursa increases impingement between the acromion and the insertion of rotator cuff tendons.
Neer (1983) described the condition in which the supraspinatus muscle impinges against the anterior edge of the acromion as subacromial impingement. Bigliani et al. (1986) and Edelson and Taitz (1992) suggested that impingement may be caused by an acromion of abnormal shape. Others have suggested that impingement lesions occur secondary to instability of the humeroscapular joint (Warren 1983, Jobe and Kvitne 1989, Nirschl 1989, Warner et al. 1990, Hawkins and Mohtadi 1991, Fu et al. 1991, Allegrucci et al. 1994).
Rotator cuff tears often cause subacromial bursitis (Fukuda et al. 1994, Payne et al. 1997, Uhthoff and Sano 1997). Many surgeons operating on the rotator cuff have found adhesion of the subacromial bursa because of bursitis (Fukuda et al. 1994, Payne et al. 1997). The present study aimed to determine whether adhesion of the subacromial bursa can cause impingement. We therefore measured the subacromial pressures before and after release of adhesion of this bursa in patients with rotator cuff tears.
Patients and Methods
In the period from 1999 to 2000, we recorded in our institution subacromial pressures during rotator cuff repair in 18 shoulders of 18 patients (10 women), having a mean age 62 (53–71) years. They had adhesions involving entire area of the subacromial bursa—i.e., between the rotator muscles and deltoid muscle and between the supraspinatus and coracoacromial ligaments. Informed consent was obtained from each patient. 8 patients reported previous shoulder trauma. The mean duration of symptoms was 12 (2–60) months. The mean UCLA score (Kay and Amstutz 1988) before surgery was 14 (11–18) points. Limitation in the range of shoulder motion was not very severe before surgery. Rotator cuff tears were full thickness in 16 patients and partial thickness in 2 (Table).
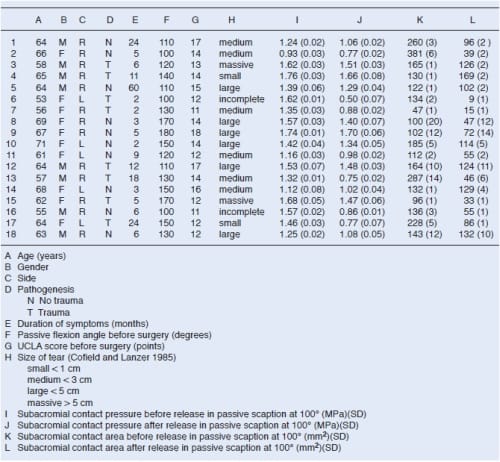
Data in 18 patients
The same surgeon (KS) operated on all patients. They were given general anesthesia with endotracheal intubation and placed in the beach chair position. A longitudinal incision from the tip of the acromion down the lateral aspect of the arm was made. The deltoid muscle and surface of the subacromial bursa were split in the direction of the fibers.
At first, the adhesion of the subacromial bursa was released only to make space for the pressure measurement film (Prescale LLW; Fuji Photo Film Co. Ltd, Tokyo, Japan (Takahashi et al. 1997)). This film, covered with a waterproof package sterilized by ethylene oxide gas, was inserted into the subacromial space (Figure 1). The film and waterproof package were 240 µm thick. The pressure measurement film itself measured 2.5 × 3.5 cm in area and was 200 µm thick. It consisted of two separately-coated sheets in apposition. The coatings consisted of two types of microcapsules, each measuring a maximum of 20 µm in diameter. Contact between the sheets caused the microcapsules to record a change in the intensity of the red color in proportion to the contact pressure. The film registered pressures from 0.5 to 2.5 MPa.
The film was inserted with the arm at the side of the body in neutral rotation and the palms facing the thigh (zero starting position); the film was then removed to evaluate the pressure in this position and a new film was inserted. The upper arm was placed in passive scaption (scapular plane elevation) at 100° (measured with a goniometer) with neutral rotation centering the humeral head around the glenoid fossa. The arm was then returned to the zero starting position and the film removed.
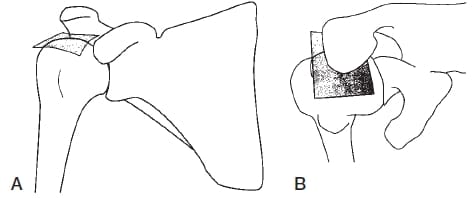
Figure 1. Figures showing frontal (A) and upper views (B) for measuring subacromial pressure. The pressure measurement film was inserted into the subacromial space.
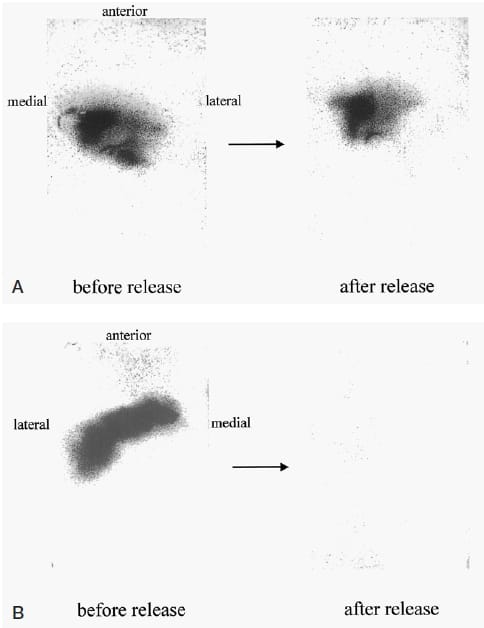
Figure 2. Photographs showing the subacromial pressure measurement films in case 1 (A) and case 2 (B) before and after release of the subacromial bursa in passive scaption at 100°. The darker color at each point indicates a higher pressure.
Adhesion of the entire area of the subacromial bursa was then released completely, either manually or with forceps and gauze. The subacromial pressure was again measured in each patient after release of the adhesion. The same procedure was repeated and a new film was used for each measurement. In this way subacromial pressures were measured 4 times in every shoulder: in the zero starting position before release, in passive scaption at 100° before release, in the zero starting position after release, and in passive scaption at 100° after release.
We used an FPD-901E analyzer (Fuji Film Prescale Pressure Measurement System, Fuji Photo Film Co Ltd, Tokyo, Japan) to evaluate the pressure recorded by the film. The mean pressure of a circle with a radius of 1 mm centered at the point of highest pressure, we called the subacromial contact pressure. The total area of contact with pressure greater than 0.5 MPa, we called the subacromial contact area. We calculated the mean of 3 analyses for 1 film. The means of 3 analyses of each contact pressure and contact area taken on each patient before or after release, we called the mean subacromial contact pressure and the mean subacromial contact area, respectively. A paired Student’s t-test was used to assess significant differences.
Results
Subacromial contact pressure
In the zero starting position before and after release of adhesion of the subacromial bursa, the subacromial contact pressure was lower than 0.5 MPa in all patients. In passive scaption at 100°, the mean subacromial contact pressure declined from 1.43 (0.93–1.76, SD 0.23) MPa before release to 1.14 (0.50–1.70, SD 0.35) MPa after release (p < 0.001).
Subacromial contact area
In the zero starting position before and after release of adhesion of the subacromial bursa, the subacromial contact area was 0 mm2 in all patients. In passive scaption at 100°, the mean subacromial contact area declined from 160 (47–381, SD 81) mm2 before release to 80 (9–169, SD 46) mm2 after release in all patients (p < 0.001).
Discussion
Before this study, to analyze the reproducibility of our methods of measurement, we made 10 measurements in one patient. In passive scaption at 100°, the mean subacromial contact pressure was 1.21 (SD 0.08) MPa. The subacromial contact area was 89 (SD 7) mm2. The tolerance interval (mean ± 2SD) was small enough to ensure that our method was accurate and reproducible.
There have been several reports of subacromial pressures measured intraoperatively in patients with rotator cuff tears. The mean pressure in hyperscaption was higher than in any other position (Jalovaara and Lantto 1992). The pressure after acromioplasty decreased significantly (Nordt et al. 1999). In our study, the mean subacromial contact pressure in passive scaption at 100° was also higher than in the zero starting position. In the zero starting position, the subacromial contact pressure and area were almost zero before and after release. This suggests that impingement may be caused by scaption in patients with adhesion of the subacromial bursa. The pressures we recorded were higher than in previous reports. We believe that this discrepancy is probably due to differences in methods of measurement and patient populations. The measurements using the pressure-sensitive film can be assumed to be much better at including pressures throughout the subacromial space and be far more sensitive to small areas of increased pressure, than bulkier catheter or transducer systems. Moreover, we studied patients with adhesion of the subacromial bursa, instead of cadavers.
We have found no reports on subacromial pressures or contact areas in patients with adhesion of the subacromial bursa. In our study, the mean subacromial contact pressure and the mean subacromial contact area declined significantly after release of the subacromial adhesion in passive scaption at 100°. These findings support our hypothesis that adhesion of the subacromial bursa enhances impingement between the acromion and the insertion of the rotator cuff tendon. Adhesion of the subacromial bursa may disturb the smooth movement of the humeral head, and fibrosis of the subacromial bursa may act as a resilient force when the shoulder is raised, because the humeral head is drawn to the acromion. Therefore, adhesion of this bursa may aggravate impingement. These changes may exacerbate tearing of the rotator cuff tendons and other degenerations, so that small tears become large ones. We suggest that in operations to repair rotator cuff tears, adhesions of the subacromial bursa should be released completely. We believe that also in subacromial bursitis without a rotator cuff tear (Neer 1983), the adhesion of the subacromial bursa may increase the subacromial pressure and enhance impingement.
References
- Allegrucci M, Whitney S L, Irrgang J. Clinical implications of secondary impingement of the shoulder in freestyle swimmers. J Orthop Sports Phys Ther 1994; 20: 307-18. Bigliani L U, Morrison D, April E W. The morphology of the acromion and its relationship to rotator cuff tears. Orthop Trans 1986; 10: 228.
- Cofield R , Lanzer W L. Pathology of rotator cuff tearing and methods of tendon repair (abstract). Orthop Trans 1985; 9: 42.
- Edelson J G, Taitz C. Anatomy of the coraco-acromial arch. Relation to degeneration of the acromion. J Bone Joint Surg (Br) 1992; 74: 589-94.
- Fu F H, Harner C D, Klein A H. Shoulder impingement syndrome. A critical review. Clin Orthop 1991; 269: 162-73.
- Fukuda H, Hamada K, Nakajima T, Tomonaga A. Pathology and pathogenesis of the intratendinous tearing of the rotator cuff viewed from en block histologic sections. Clin Orthop 1994; 304: 60-7.
- Hawkins R J, Mohtadi N G H. Controversy in anterior shoulder instability. Clin Orthop 1991; 272: 152-62. Jalovaara P, Lantto V. Local pressures in subacromial space at different positions of the humerus. Acta Orthop Scand (Suppl 247) 1992; 63: 23-4.
- Jobe F W, Kvitne R S. Shoulder pain in the overhand or throwing athlete: The relationship of anterior instability and rotator cuff impingement. Orthop Rev 1989; 18: 963-75.
- Kay S, Amstutz H C. Shoulder hemiarthroplasty at UCLA. Clin Orthop 1988; 228: 42-4.
- Neer C S. Impingement lesions. Clin Orthop 1983; 173: 70-7.
- Nirschl R P. Rotator cuff tendinitis. Basic concepts of pathoetiology. Instructional Course Lectures 1989; 38: 439-45.
- Nordt W E, Garretson R B, Plotkin E. The measurement of subacromial contact pressure in patients with impingement syndrome. Arthroscopy 1999; 15: 121-5.
- Payne L Z, Altchek D W, Craig E V, Warren R F. Arthroscopic treatment of partial rotator tears in young athletes. Am J Sports Med 1997; 25: 299-305.
- Takahashi T, Wada Y, Yamamoto H. Soft-tissue balancing with pressure distribution during total knee arthroplasty. J Bone Joint Surg (Br) 1997; 79: 235-9.
- Uhthoff H K, Sano H. Pathology of failure of the rotator cuff tendon. Orthop Clin North Am 1997; 28: 31-41.
- Warner J J P, Micheli L J, Arslanian L E, Kennedy J, Kennedy R. Patterns of flexibility, laxity, and strength in normal shoulders and shoulders with instability and impingement. Am J Sports Med 1990; 18: 366-75.
- Warren R F. Subluxation of the shoulder in athletes. Clin Sports Med 1983; 2: 339-54.
